Citation, DOI, disclosures and article data
Citation:
Knipe H, Recurrent carpal tunnel syndrome. Reference article, Radiopaedia.org (Accessed on 20 Mar 2025) https://doi.org/10.53347/rID-178332
Disclosures:
At the time the article was created Henry Knipe had the following disclosures:
- Integral Diagnostics, Shareholder (ongoing)
- Micro-X Ltd, Shareholder (ongoing)
These were assessed during peer review and were determined to
not be relevant to the changes that were made.
View Henry Knipe's current disclosures
Disclosures:
At the time the article was last revised Henry Knipe had the following disclosures:
- Integral Diagnostics, Shareholder (ongoing)
- Micro-X Ltd, Shareholder (ongoing)
These were assessed during peer review and were determined to
not be relevant to the changes that were made.
View Henry Knipe's current disclosures
Recurrent carpal tunnel syndrome is the persistence or re-occurrence of carpal tunnel syndrome (CTS) symptoms after carpal tunnel release surgery.
The re-operation rate for new or persistent CTS symptoms is 1-3% 1-3.
Persistence or re-occurrence of CTS symptoms may be due to 1-3:
incorrect pre-operative diagnosis, e.g. more proximal median nerve entrapment syndrome, brachial neuritis, thoracic outlet syndrome, nerve tumour, cervical radiculopathy, multiple sclerosis, peripheral neuropathies (from various causes)
-
incomplete release of the flexor retinaculum
-
nerve tethering/fibrosis
circumferentially around the nerve or adherence to the radial wall of the carpal tunnel
re-occurrent symptoms after initial improvement
second most common cause found on revision carpal tunnel release
unrecognised carpal tunnel compressive lesions, e.g. flexor tenosynovitis, mass lesion, accessory muscle belly
iatrogenic nerve injury: may be incomplete or complete laceration
permanent nerve damage from chronic and severe compression
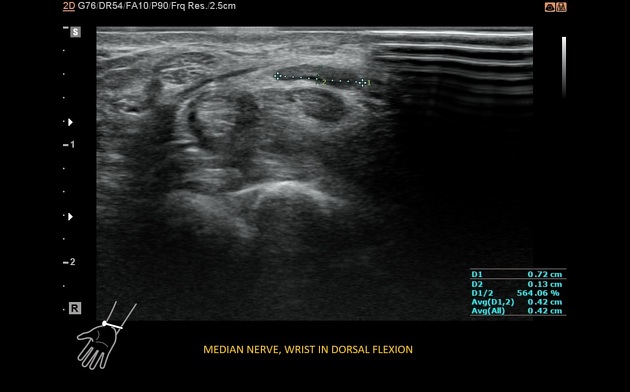
Ultrasound
detection of focal (more common) or longitudinal compression and site (i.e. proximal, mid, distal carpal tunnel) of compression 4
persistence of the flexor retinaculum 4, although transducer compression can cause overlap of a transected flexor retinaculum 5
absence of nerve gliding indicates perineural fibrosis, lateral gliding is easier to assess than longitudinal gliding 4
Treatment and prognosis
Response to a steroid injection around the median nerve can be considered a predictor for successful revision carpal tunnel release 1,3.
-
1. Van M, Jose R, Power D. Failed Carpal Tunnel Surgery: A Guide to Management. J Musculoskelet Surg Res. 2019;3(1):30. doi:10.4103/jmsr.jmsr_78_18 - Pubmed
-
2. Neuhaus V, Christoforou D, Cheriyan T, Mudgal C. Evaluation and Treatment of Failed Carpal Tunnel Release. Orthop Clin North Am. 2012;43(4):439-47. doi:10.1016/j.ocl.2012.07.013 - Pubmed
-
3. Zhang D, Earp B, Blazar P. Evaluation and Management of Unsuccessful Carpal Tunnel Release. J Hand Surg Am. 2019;44(9):779-86. doi:10.1016/j.jhsa.2019.05.018 - Pubmed
-
4. Carità E, Donadelli A, Laterza M, Perazzini P, Tamburin S, Zanette G. High-Resolution Ultrasound in the Diagnosis of Failed Carpal Tunnel Decompression: A Study of 35 Cases. J Hand Surg Eur Vol. 2022;47(4):364-8. doi:10.1177/17531934211068636 - Pubmed
-
5. Chen C, Jaw F, Hu J, Wu W, Chang K. Dynamic Ultrasound for Evaluating the Adequacy of Median Nerve Decompression Following Minimally Invasive Carpal Tunnel Release: Technical Innovation and Case Study. Heliyon. 2023;9(1):e13107. doi:10.1016/j.heliyon.2023.e13107 - Pubmed
Promoted articles (advertising)




 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.