
Renal artery aneurysms (RAA) are the second most common visceral aneurysms (15-22%), the most common being splenic artery aneurysms (60%).
On this page:
Epidemiology
Renal artery aneurysms occur in ~0.1% of the population 6,8,10. They are more common in females 6. The median age at diagnosis is 50 years 8.
Clinical presentation
Most cases are asymptomatic. Symptoms usually arise from aneurysm rupture, peripheral vascular bed embolization, or arterial thrombosis 1. Hypertension is associated with ~70% (range 67-75%) 10. Hematuria has also been reported in many cases.
In pregnancy, the acute, severe unilateral flank pain induced by maternal renal artery aneurysm rupture is usually attributed to several other, more common causes. This explains in part the high maternal and fetal mortality rate, which is why it should always be on the list of differential diagnoses, especially if followed by dropping blood pressure 9.
Pathology
Approximately 20% of cases are bilateral. Most aneurysms are saccular and tend to occur at the bifurcation of the main renal artery or first-order branch 8.
Etiology
fibromuscular dysplasia (FMD): 35%
degenerative aneurysm: 25%
vasculitides, e.g. Behcet disease
intrinsic collagen deficiency, e.g. Marfan syndrome, Ehlers-Danlos syndrome
trauma 1,2
Radiographic features
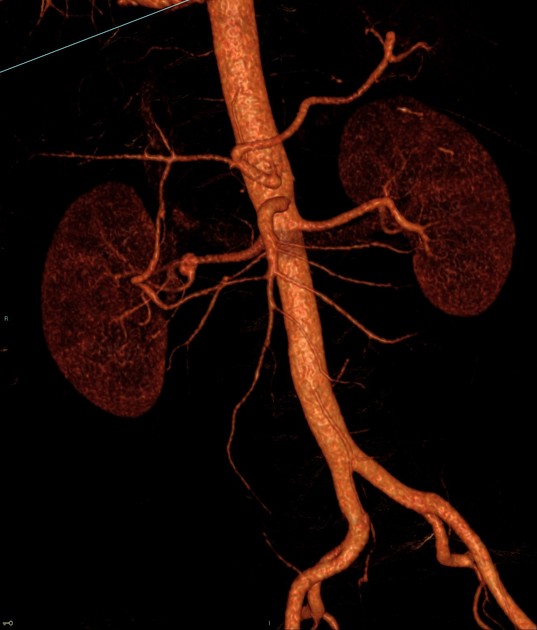
CT angiography is recommended as the modality of choice for assessing renal artery aneurysms 10.
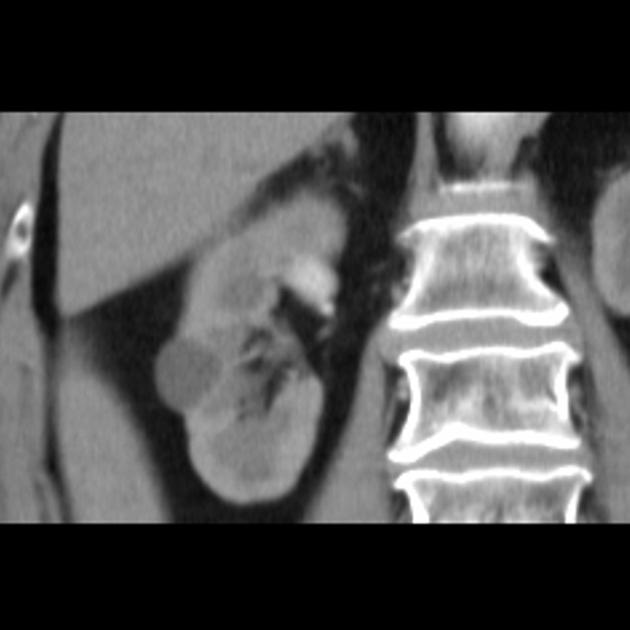
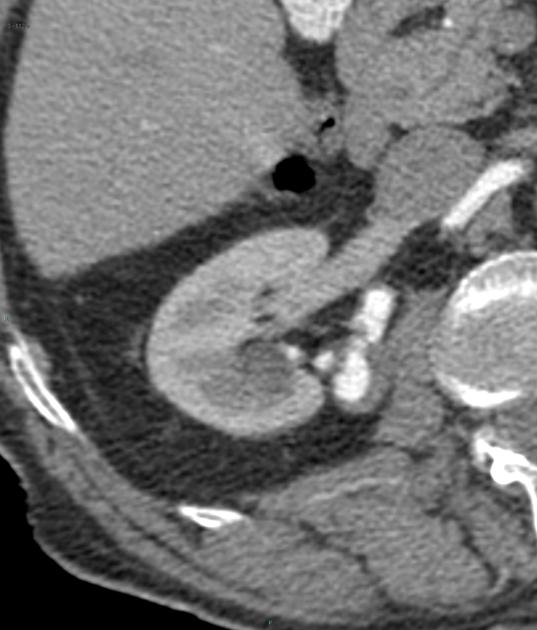
CT
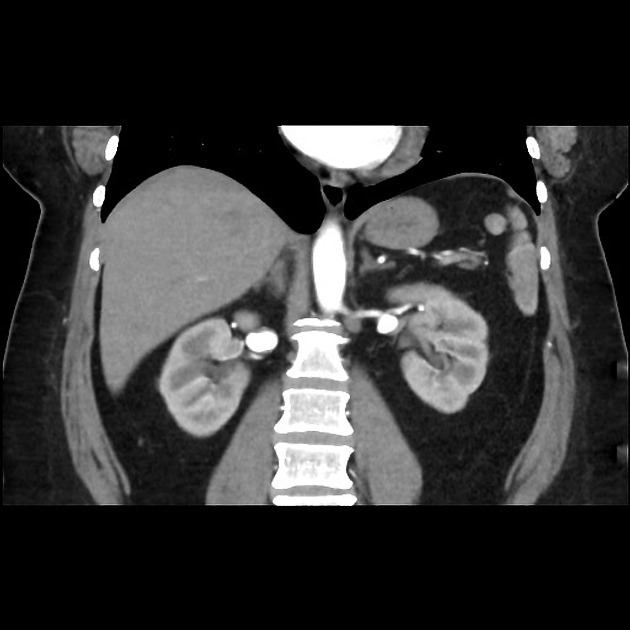
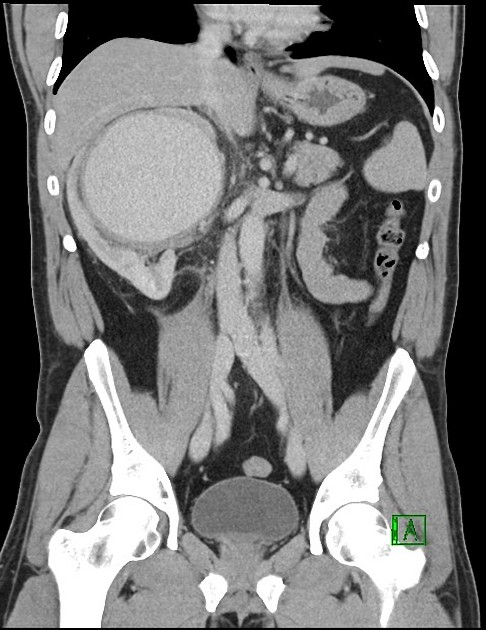
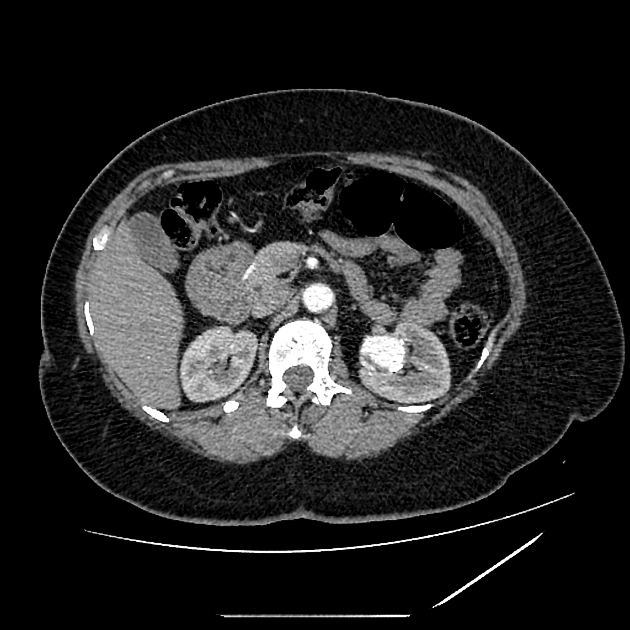
non-contrast: soft tissue mass lesion in the region or course of renal artery
post-contrast: contrast-filled outpouching in the course of the renal artery
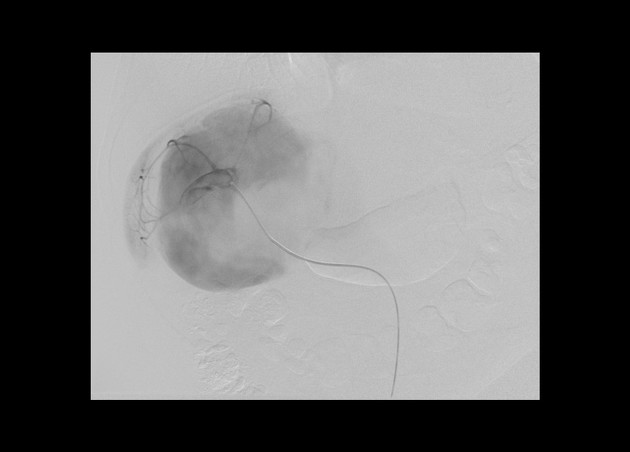
Angiography (DSA)
Aneurysms can be well detected and characterized by angiography, in terms of size, neck diameter and type.
Treatment and prognosis
Renal artery aneurysms grow slowly if at all 10. Rupture rates are estimated to be ~4% (range 3-5%) with the mortality rate in the general population being ~10% 10. Pregnancy-associated rupture is associated with very high mortality rates for both mother (~55%) and fetus (~85%) 10.
The Society for Vascular Surgery 2020 guidelines recommend 10:
-
surgical management of renal artery aneurysms >3 cm
open surgical reconstructive technique preferred for non-complex renal artery aneurysms
ex vivo repair and autotransplatation preferred over nephrectomy for complex renal artery aneurysms (e.g distal or parenchymal aneurysms)
stent graft exclusion or embolization in patients high peri-operative risk
symptomatic or ruptured aneurysms
renal artery anerusyms of any size in patients who have childbearing potential
renal artery aneurysms of any size in patients with treatment-resistant hypertension and significant renal artery stenosis
for non-surgically managed patients, annual surveillance imaging until stable size on two consecutive studies, then surveillance imaging every 2-3 years








 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.