
The American Association for the Surgery of Trauma (AAST) renal injury scale, updated in 2018, is the most widely used grading system for renal trauma.
The 2018 update incorporates "vascular injury" (i.e. pseudoaneurysm, arteriovenous fistula) into the imaging criteria for visceral injury.
On this page:
Classification
Severity is assessed according to the depth of renal parenchymal damage and involvement of the urinary collecting system and renal vessels.
-
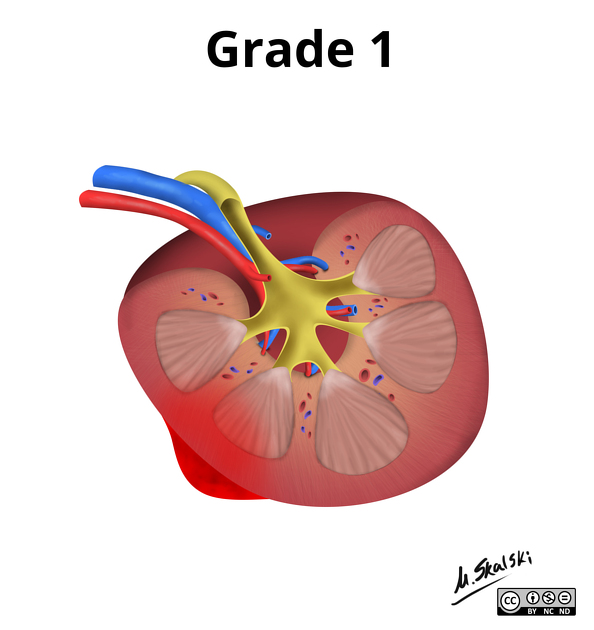
grade I
subcapsular haematoma and/or contusion, without laceration
-
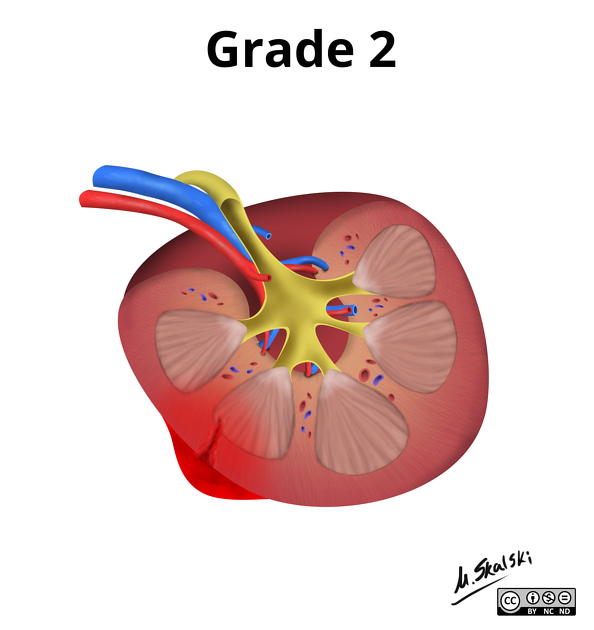
grade II
superficial laceration ≤1 cm depth not involving the collecting system (no evidence of urine extravasation)
perirenal haematoma confined within the perirenal fascia
-
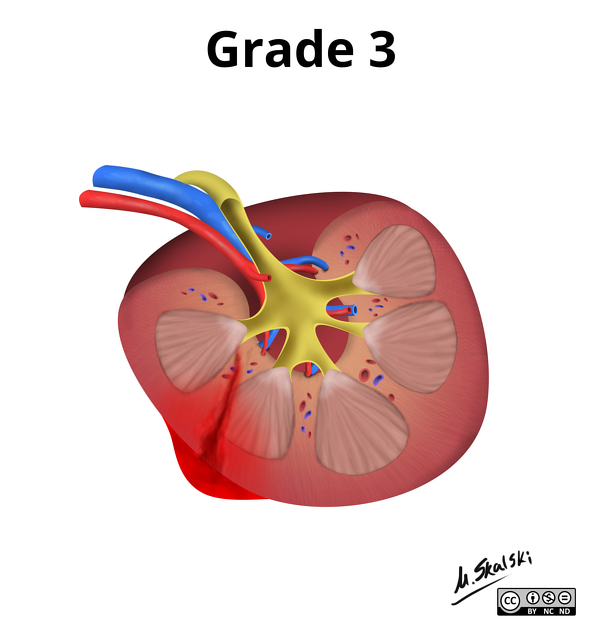
grade III
laceration >1 cm not involving the collecting system (no evidence of urine extravasation)
vascular injury or active bleeding confined within the perirenal fascia
-
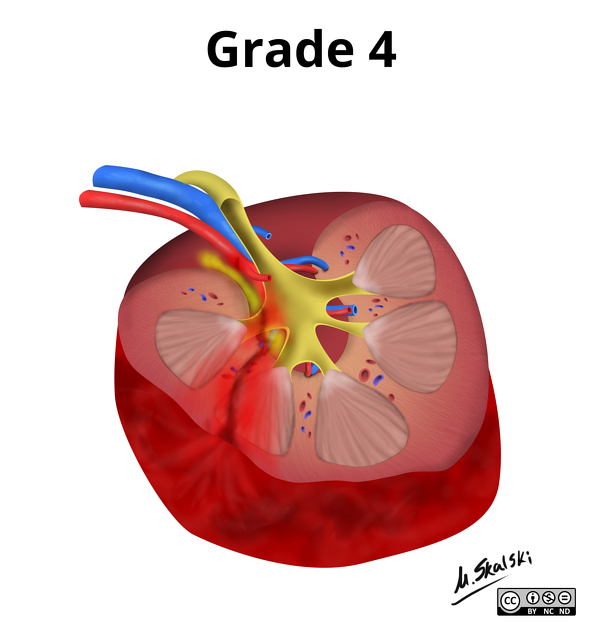
grade IV
laceration involving the collecting system with urinary extravasation
laceration of the renal pelvis and/or complete ureteropelvic disruption
vascular injury to segmental renal artery or vein
segmental infarctions without associated active bleeding (i.e. due to vessel thrombosis)
active bleeding extending beyond the perirenal fascia (i.e. into the retroperitoneum or peritoneum)
-
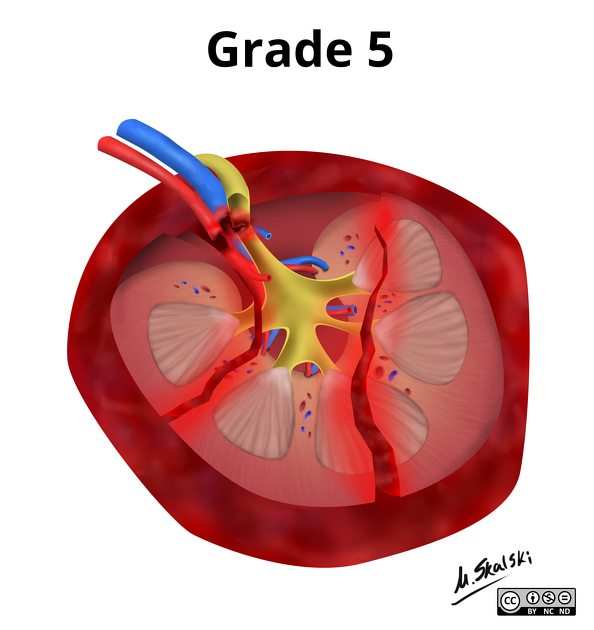
grade V
shattered kidney
avulsion of renal hilum or laceration of the main renal artery or vein: devascularisation of a kidney due to hilar injury
devascularised kidney with active bleeding
Additional points
advance one grade for multiple injuries up to grade III
vascular injury (i.e. pseudoaneurysm or AV fistula): appears as a focal collection of vascular contrast which decreases in attenuation on delayed images
active bleeding: focal or diffuse collection of vascular contrast which increases in size or attenuation on a delayed phase
Imaging technique
The AAST guidelines recommend dual arterial/portal venous phase imaging for evaluation of a vascular injury of liver, spleen, or kidney 8.
If there are imaging or clinical findings suggesting collecting system injury (e.g. haematuria or blood at the meatus), additional delayed excretory phase images should be obtained after 5-15 minutes of delay to evaluate for urine extravasation 5,8. Urinary contrast is usually hyperdense and readily distinguished from haemorrhagic vascular contrast.
Note that multiphase scanning should not preempt emergent management in the setting of haemodynamic instability or other life-threatening injuries.
Treatment and prognosis
grade I: conservative management
grade II: conservative management under close observation
grade III: conservative management under close observation; may be managed surgically if undergoing laparotomy for other abdominal injuries
grade IV: surgical management, especially if undergoing laparotomy for other abdominal injuries
grade V: surgical management
Complications
grade IV renal injury places the patient at risk for developing hypertension due to a decrease in the renal blood flow or secondary to compression of the renal vessels (see Page kidney), leading to an activation of the renin-angiotensin system
External links
If any of these links are broken or for other problems and questions, please contact editors@radiopaedia.org.













 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.