Rhinoscleroma
Updates to Article Attributes
Rhinoscleroma is a chronic granulomatous infection involving the upper respiratory tract due to Klebsiella rhinoscleromatis. It initially involves the nasal mucosae but it may progress to any other part of the upper respiratory tract.
Untreated rhinoscleroma slowly progresses over many years 1.
Clinical presentation
Patients most often present with nasal obstruction. Other nonspecific symptoms are often encountered such as epistaxis, rhinorrhea, dysphagia, stridor, and dysphonia.
Epidemiology
Patients with rhinoscleroma are usually between 10 to 30 years old. Poor hygiene, prolonged close contact, and malnutrition are considered risk factors. It is endemic in Central America, Egypt, tropical Africa, India, and Indonesia 3.
Radiographic features
The mainCharacteristic radiological feature of rhinoscleroma is focalthe presence of nasal mass with the following criteria; 4, 5
CT
-
bilateral or
diffuse trachealunilateral expansile nasal masses, lesions are usually homogeneous, hyperdense and non-enhancing - masses usually extend through the nasal nare anteriorly and into the adjacent paranasal sinuses
-
lesions line the sinus wall
thickeningcausing bone sclerosis, bone thinning (pressure atrophy) or it may absorb it withor without nodularity. Hence,extra-sinus extension -
no bone destruction which helps to differentiate it
also presentsfrom malignant lesions -
in longstanding cases, rhinoscleroma may extend to involve other parts of the upper respiratory tract, such as
subglottic stricturephayrnx with nodular infiltration of the orophayrnx, tonsillar bed, soft and hard palate. It may also show laryngotracheal involvement, the usual site of laryngeal involvement is the glottic–subglottic region showing concentric narrowing of thetrachea. Theairway, thickeningisof the tracheal wall and nodular thickening ofsoft-tissue densitythe tracheal mucosa 5
MRI
lesions demonstrate characteristic signal intensity 4,5:
T1: mild to marked high signal intensity secondary to increased protein content within Mikulicz cells and Russel bodies
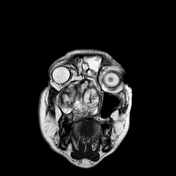
T2: hyperintense due to its high cellular component with hypointense foci of fibrosis
T1 C+ (Gd): inhomogeneous contrast enhancement secondary to areas of fibrosis.
DWI: diffusion restriction with low apparent diffusion coefficients values secondary to high cellularity, without calcifications 1.
Differential diagnosis
For aThe differential diagnosis of nasal masses includes granulomatous and neoplastic diseases which can mimic rhinoscleroma, see 5
Granulomatous diseases include:
-
infectious granulomatous processes:
- bacterial (tuberculosis, actinomycosis, leprosy, and syphilis),
- fungal (histoplasmosis, sporotrichosis, paracoccidioidomycosis)
- parasitic (mucocutaneous leishmaniasis)
- noninfectious granulomatous diseases (granulomatosis with polyangiitis and sarcoidosis)
Neoplasms: such as(lymphoma and sinonasal carcinoma). Expansion of the nasal cavities, scalloping of the sinus wall, lack of bone destruction and hyperintensity on T1 help to differentiate rhinoscleroma from nasal malignancies
Differential diagnosis for tracheal subglottic narrowing include:
- diffuse tracheal narrowing
- focal thickening of the tracheal wall
-<p><strong>Rhinoscleroma </strong>is a chronic granulomatous infection involving the upper respiratory tract due to <em>Klebsiella rhinoscleromatis</em>. It initially involves the nasal mucosae but it may progress to any other part of the upper respiratory tract.</p><p>Untreated rhinoscleroma slowly progresses over many years <sup>1</sup>.</p><h4>Clinical presentation</h4><p>Patients most often present with nasal obstruction. Other nonspecific symptoms are often encountered such as epistaxis, rhinorrhea, dysphagia, stridor, and dysphonia.</p><h4>Epidemiology</h4><p>Patients with rhinoscleroma are usually between 10 to 30 years old. Poor hygiene, prolonged close contact, and malnutrition are considered risk factors. It is endemic in Central America, Egypt, tropical Africa, India, and Indonesia <sup>3</sup>.</p><h4>Radiographic features</h4><p>The main feature of rhinoscleroma is focal or diffuse tracheal wall thickening with or without nodularity. Hence, it also presents as subglottic stricture and narrowing of the trachea. The thickening is of soft-tissue density, without calcifications <sup>1</sup>.</p><h4>Differential diagnosis</h4><p>For a differential diagnosis, see :</p><ul>- +<p><strong>Rhinoscleroma </strong>is a chronic granulomatous infection involving the upper respiratory tract due to <em>Klebsiella rhinoscleromatis</em>. It initially involves the nasal mucosae but it may progress to any other part of the upper respiratory tract.</p><p>Untreated rhinoscleroma slowly progresses over many years <sup>1</sup>.</p><h4>Clinical presentation</h4><p>Patients most often present with nasal obstruction. Other nonspecific symptoms are often encountered such as epistaxis, rhinorrhea, dysphagia, stridor, and dysphonia.</p><h4>Epidemiology</h4><p>Patients with rhinoscleroma are usually between 10 to 30 years old. Poor hygiene, prolonged close contact, and malnutrition are considered risk factors. It is endemic in Central America, Egypt, tropical Africa, India, and Indonesia <sup>3</sup>.</p><h4>Radiographic features</h4><p>Characteristic radiological feature of rhinoscleroma is the presence of nasal mass with the following criteria; <sup>4, 5</sup></p><h6>CT</h6><ul>
- +<li>bilateral or unilateral expansile nasal masses, lesions are usually homogeneous, hyperdense and non-enhancing</li>
- +<li>masses usually extend through the nasal nare anteriorly and into the adjacent paranasal sinuses</li>
- +<li>lesions line the sinus wall causing bone sclerosis, bone thinning (pressure atrophy) or it may absorb it with extra-sinus extension</li>
- +<li>no bone destruction which helps to differentiate it from malignant lesions</li>
- +<li>in longstanding cases, rhinoscleroma may extend to involve other parts of the upper respiratory tract, such as phayrnx with nodular infiltration of the orophayrnx, tonsillar bed, soft and hard palate. It may also show laryngotracheal involvement, the usual site of laryngeal involvement is the glottic–subglottic region showing concentric narrowing of the airway, thickening of the tracheal wall and nodular thickening of the tracheal mucosa <sup>5</sup>
- +</li>
- +</ul><h6>MRI</h6><p>lesions demonstrate characteristic signal intensity <sup>4,5</sup>:</p><p><strong>T1:</strong> mild to marked high signal intensity secondary to increased protein content within Mikulicz cells and Russel bodies</p><p><strong>T2:</strong> hyperintense due to its high cellular component with hypointense foci of fibrosis</p><p><strong>T1 C+ (Gd):</strong> inhomogeneous contrast enhancement secondary to areas of fibrosis.</p><p><strong>DWI:</strong> diffusion restriction with low apparent diffusion coefficients values secondary to high cellularity, which could mimic malignancy</p><h4>Differential diagnosis</h4><p>The differential diagnosis of nasal masses includes granulomatous and neoplastic diseases which can mimic rhinoscleroma, <sup>5</sup></p><p><strong>Granulomatous diseases</strong> include:</p><ul>
- +<li>infectious granulomatous processes:<ul>
- +<li>bacterial (<a href="/articles/tuberculosis">tuberculosis</a>, actinomycosis, <a href="/articles/leprosy">leprosy</a>, and syphilis),</li>
- +<li>fungal (histoplasmosis, sporotrichosis, paracoccidioidomycosis)</li>
- +<li>parasitic (<a href="/articles/leishmaniasis">mucocutaneous leishmaniasis</a>)</li>
- +</ul>
- +</li>
- +<li>noninfectious granulomatous diseases (<a href="/articles/granulomatosis-with-polyangiitis-upper-respiratory-tract-manifestations-2">granulomatosis with polyangiitis </a>and <a href="/articles/sarcoidosis-head-and-neck-manifestations-1">sarcoidosis</a>)</li>
- +</ul><p><strong>Neoplasms: </strong>such as<strong> </strong>(<a href="/articles/sinonasal-lymphoma">lymphoma</a> and <a href="/articles/sinonasal-adenocarcinoma">sinonasal carcinoma</a>). Expansion of the nasal cavities, scalloping of the sinus wall, lack of bone destruction and hyperintensity on T<sub>1</sub> help to differentiate rhinoscleroma from nasal malignancies</p><p>Differential diagnosis for tracheal subglottic narrowing include:</p><ul>
References changed:
- 4. Ahmed Abdel Khalek Abdel Razek, Ahmed Ahmed Elasfour. MR Appearance of Rhinoscleroma. (1999) American Journal of Neuroradiology. 20 (4): 575. <a href="https://www.ncbi.nlm.nih.gov/pubmed/10319963">Pubmed</a> <span class="ref_v4"></span>
- 5. Dalia Ibrahim, Ahmed Fayed. Report of a case of giant rhinoscleroma: CT and MRI. (2018) BJR|case reports. 4 (4): 20180027. <a href="https://doi.org/10.1259/bjrcr.20180027">doi:10.1259/bjrcr.20180027</a> - <a href="https://www.ncbi.nlm.nih.gov/pubmed/30931141">Pubmed</a> <span class="ref_v4"></span>
Image 1 CT (C+ portal venous phase) ( create )

Image 2 MRI (T2) ( create )