
A sinus of Valsalva aneurysm refers to abnormal dilatation of the sinus of valsalva and is a cause of thoracic aortic dilatation. Sinus of Valsalva aneurysms arise from one of the aortic sinuses. They are either congenital or acquired.
On this page:
Epidemiology
There is a male predilection (M:F ratio being around 3-4:1). They are relatively more common in eastern and Asian populations and can occur in any age group with a mean age of 35 years at presentation 4.
Associations
Commonly occur with other congenital heart anomalies, including:
Clinical presentation
They may be asymptomatic. Presentation with a catastrophic acute rupture is quite common. Dyspnoea, chest pain, palpitations, and cardiac murmurs may occur 4.
Pathology
Aetiology
Sinus of Valsalva aneurysm may be either congenital or acquired. Congenital causes include:
-
collagen vascular disease
-
vasculitis
Acquired causes include:
-
infection
iatrogenic
traumatic
Location
In congenital cases, they most often involve the right coronary sinus (70-90% 11), less frequently the non-coronary sinus (10-25%), and rarely left coronary sinus (<5%) 3,11..
Radiographic features
They are saccular and arise above the aortic annulus.
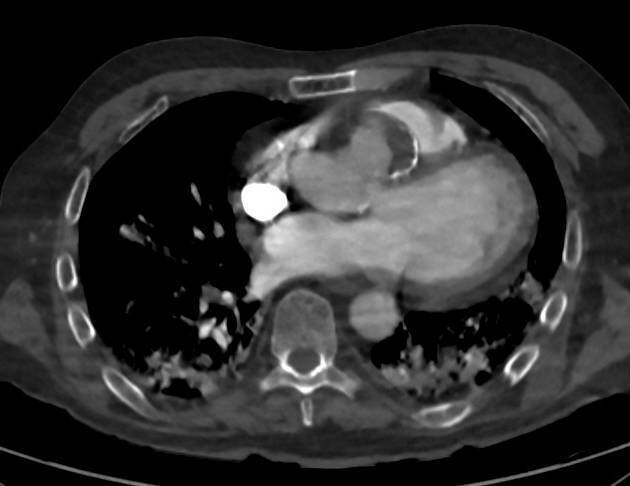
MRI/CT
MRI is considered the imaging modality of choice, especially with the mycotic type. The saccular aneurysm is seen arising from one of the sinuses (right coronary sinus being the most common location) and protruding into an adjacent cardiac chamber.
The normal sinus diameter upper limit is usually taken as 40 mm (with some publications suggesting 36 mm for females) 6.
Echocardiography
Transoesophageal echocardiography is preferred for anatomical delineation of the origin of the aneurysm, which will appear on two-dimensional imaging as a mobile, thin walled structure, circular in the short axis, protruding from above the plane of the coronary artery origins into an adjacent cardiac chamber. The appearance is classically described as a "windsock" deformity with enlargement during systole 8.
Filling of the aneurysm may be observed with colour flow Doppler, and the use of contrast may aid in the visualisation of the left-to-right shunt, as well as differentiating between ruptured and unruptured aneurysms 9. The use of spectral Doppler allows quantification of flow velocity and direction; rupture into a cardiac chamber with subsequent shunting typically yields constant flow from the aorta to the lower pressure chamber throughout the cardiac cycle, potentially allowing differentiation from other intracardiac shunts, e.g. ventricular septal defects 10.
Treatment and prognosis
Surgical repair with a Bentall procedure can be performed.
Complications
-
most commonly into right ventricle
may lead to cardiac tamponade +/- intracardiac shunting
arrhythmias




 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.