
Sinus tracts are an abnormal connection between a fluid collection with a mucous mucosal surface and/or skin 1,2. It can result from acute or chronic processes and occasionally extend into the joints and bones 1.
On this page:
Terminology
The term sinus tract is non-specific; however, when used in soft tissue or bony infections, it generally delineates the extent of infection 1. If the abnormal connection is between two epithelial surfaces such as between hollow organs, skin or vessels, the term fistula is used.
Aetiology
Sinus tracts can develop 2:
spontaneously
secondary to iatrogenic injury (e.g. surgical incision)
post-traumatic
underlying collection or necrotic material (e.g. necrotising pancreatitis)
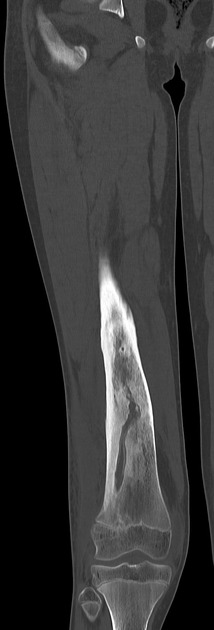
secondary to infective bone foci (e.g. osteomyelitis)
secondary to infected membranous sacs (e.g. chronic empyema)
secondary to an underlying foreign body (e.g. shrapnel)
Complications
Squamous cell carcinoma may rarely develop within the chronic sinus tracts in cases of chronic osteomyelitis 3,4.
Radiographic features
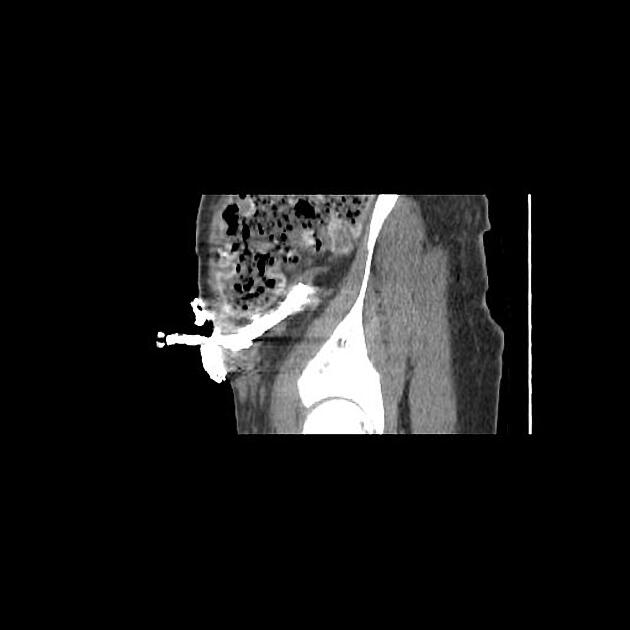
Fluoroscopy
Direct visualisation of the sinus tract, its ramifications, and extent can be done using radio-opaque contrast material under fluoroscopic guidance.
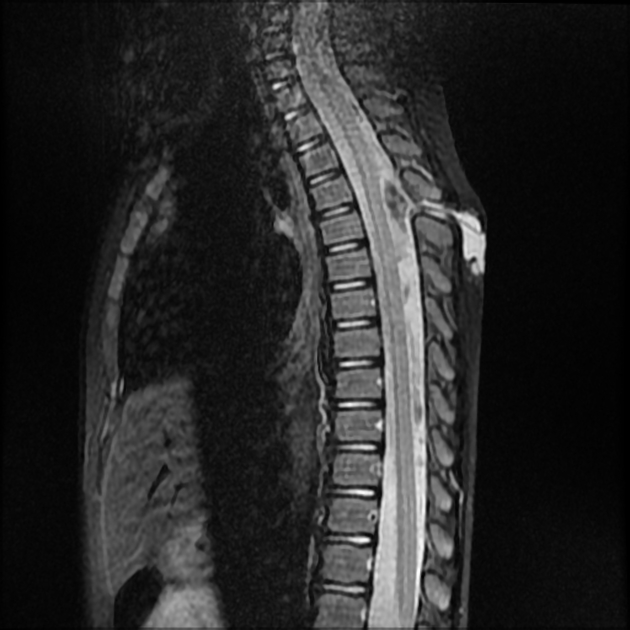
MRI
Active tracts are typically 1:
T1: hypointense
T2/T2FS: hyperintense
T1 C+: tram-track pattern of peripheral enhancement
Chronic fibrosed sinus tracts typically demonstrate T1 and T2 hypointense signals without contrast enhancement 1.
Radiological report
The radiological report should contain a description of the following:
presence, location, size, and ramifications of the sinus tract
-
associated findings
presence, location, and size of the underlying abnormal collection
extension into the joint or bone


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.