
Tornwaldt cysts (also spelled as Thornwaldt cyst or Thornwald cyst) are common incidental benign midline nasopharyngeal mucosal cysts. A symptomatic cyst is also called Tornwaldt disease 7,8.
On this page:
Epidemiology
Tornwaldt cysts are developmental and usually asymptomatic. In most cases they are found incidentally; as such, age of diagnosis typically represents age of imaging of the nasopharynx. Peak incidence has been variably reported between the ages of 15 and 60 years 1,3, which may be due to gradual accumulation of fluid in the cyst following obliteration of its neck.
Tornwaldt cysts have an autopsy prevalence of approximately 4%, with no gender predilection 3. These incidences found at autopsy studies in 1950s and 60s differ from findings in an incidence study using CT and/or MR, demonstrating an incidence of only 0.06% 7. The reason for this discrepancy is unclear.
Clinical presentation
Tornwaldt cysts are almost always asymptomatic. However, if they become infected, they can cause halitosis or periodic discharge of foul-tasting fluid into the mouth. Some may present with otitis media due to obstruction of the Eustachian tube 7,8.
Pathology
Tornwaldt cysts are classified as crusting and cystic 8. They form as a result of retraction of the notochord where it contacts with the endoderm of the primitive pharynx.
This is believed to happen at about the 10th week of embryonic development. Closure at the orifice results in the so-called cystic type, while crusts adhering to the orifice without closure result in the crust type 8. The cyst is lined by respiratory epithelium and accumulates fluid containing variable proteinaceous content. Inflammation can occur due to obstruction.
There is a report of Tornwaldt cyst formation following concurrent chemoradiotherapy for nasopharyngeal carcinoma 6.
Radiographic features
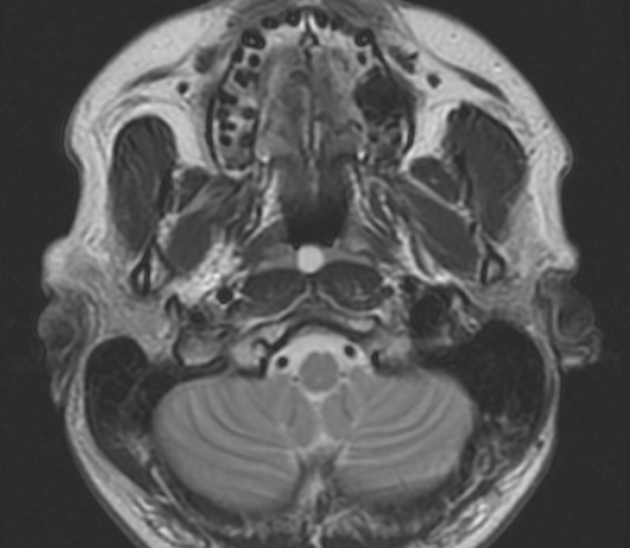
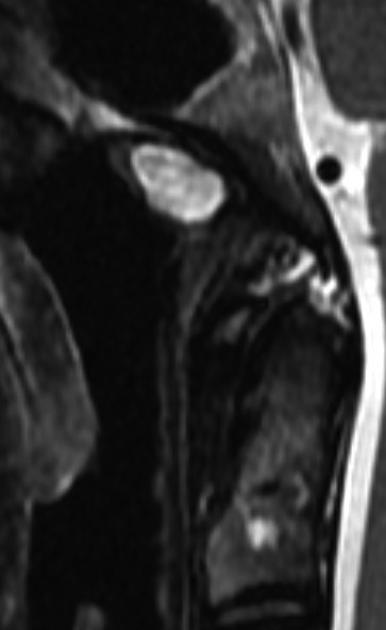
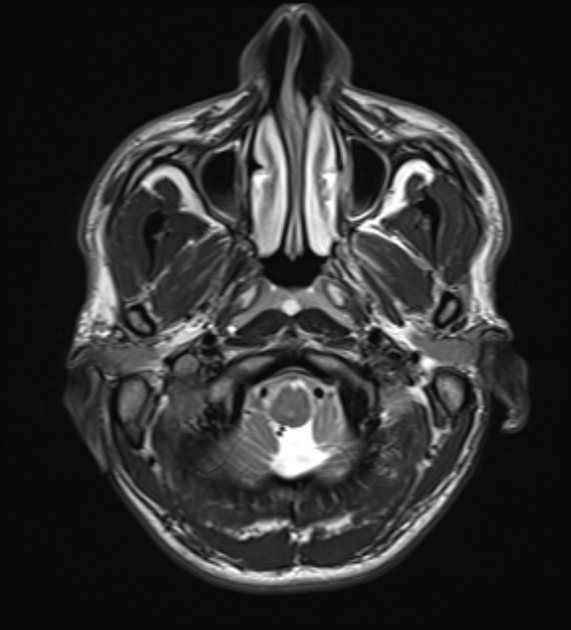
These lesions have a characteristic appearance and should usually not be confused with more sinister pathology. Typically, they are well-circumscribed rounded lesions immediately deep to the mucosa. They are usually nestled between and anterior to the longus colli muscles. They elevate the mucosa, forming a convex surface into the nasopharynx. They are variable in size, ranging from a few millimeters to a few centimeters in diameter, but are typically 2-10 mm in size 1,3.
CT
On CT they appear as well-circumscribed low density (fluid density centrally) and are non-enhancing. If the fluid is protein-rich, it may be hyperattenuating and can even mimic a solid lesion.
MRI
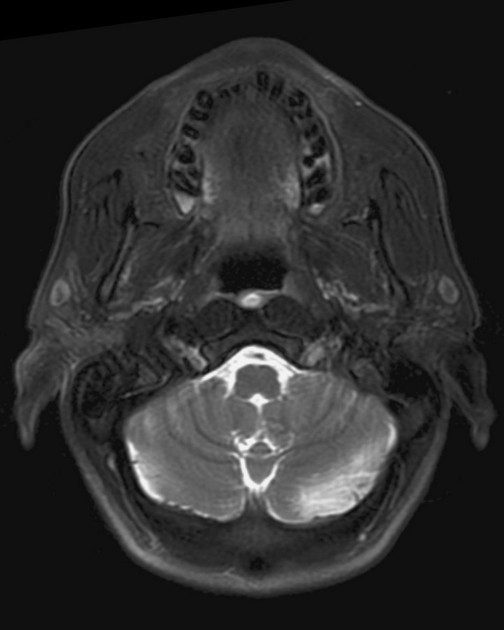
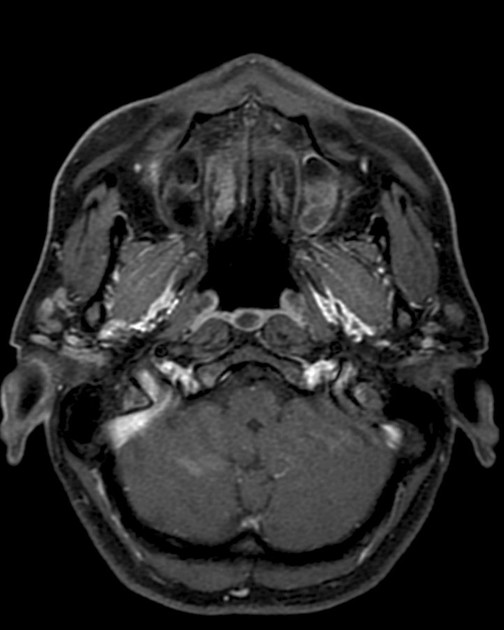
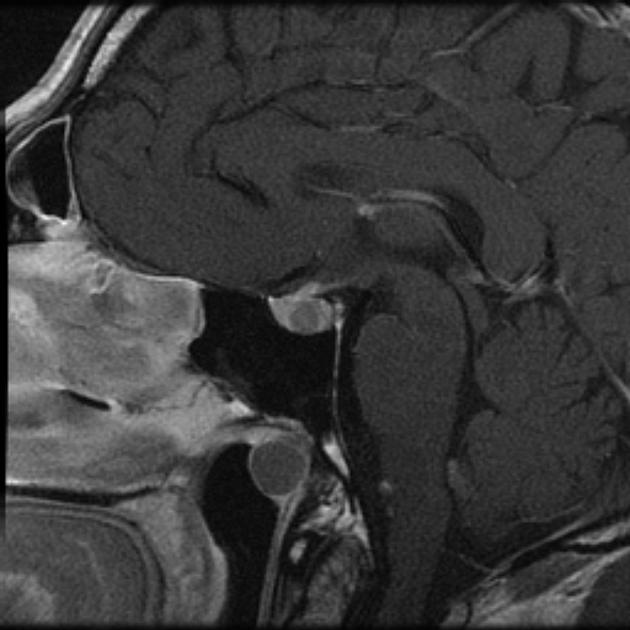
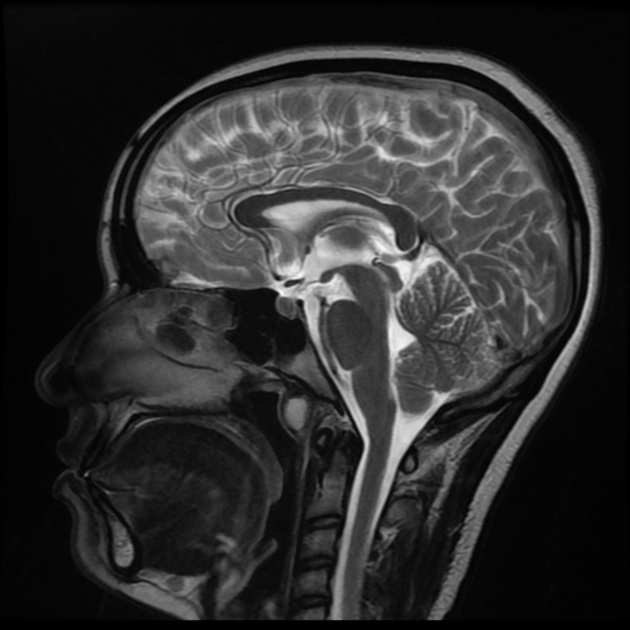
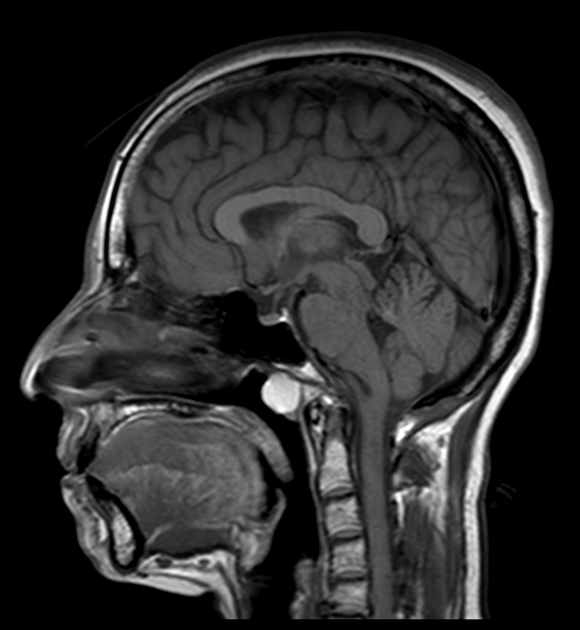
Similarly, MRI demonstrates these cysts as being well-circumscribed with a thin wall.
Signal characteristics
T1: signal is variable depending on protein content
T2: high signal
T1 C+ (Gd): no enhancement
Treatment
Asymptomatic lesions require no treatment. If treatment is required, deroofing the cyst (marsupialization) is usually sufficient and can be performed via a transnasal approach 4.
Differential diagnosis
There is usually no real differential, however adenoidal/mucosal masses can sometimes have cystic components, and therefore the differential includes:
normal/prominent adenoidal tissue
intra-adenoid cyst: can be difficult to differentiate on MRI from a Tornwaldt cyst 10
nasopharyngeal carcinoma (NPC): up to 12% are midline 2
History and etymology
It is named after Gustav Ludwig Tornwaldt (1843-1910) 5, a German physician who described it as a pathological entity in 1885 9. The original description of this cyst is thought to have been made by A F C J Meyer in 1840 9.






 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.