
Valgus instability of the elbow can develop as a result of ulnar collateral ligament injury either in the setting of chronic overuse or in the context of an acute or an acute-on-chronic injury.
On this page:
Epidemiology
Valgus instability can be seen in athletes and less commonly in non-athletes.
Risk factors
Overhead athletic activity is considered as a main predisposing factor for valgus instability including 1,2:
- throwing sports
- baseball pitching
- javelin throwing
- handball
- racket-sports
- weight-lifting
- gymnastics
Associations
Valgus instability might be associated with the following clinical conditions 2-4:
- flexor-pronator mass injury
- radiocapitellar compression fractures
- little leaguer's elbow
- medial epicondyle apophysitis
- posteromedial elbow impingement
- cubital tunnel syndrome
- elbow dislocation
Diagnosis
The diagnosis of valgus instability is primarily established clinically and requires typical findings on examination as well as clues from the patient history 2.
The moving valgus stress test is considered a highly sensitive test and moderately specific test (>99%/~75%) 5.
Imaging aids in the evaluation of the medial collateral ligament complex and can detect causative lesions such as tears, avulsion injuries and associated injuries to the radiocapitellar joint to confirm clinical findings 2,3.
MRI and MR arthrography are considered highly sensitive and specific for the detection of medial collateral ligament complex disruption 3,6.
Clinical presentation
Typical complaints in the setting of chronic valgus instability include gradually worsening or fluctuating elbow pain or progressively worsening performance specifically related to causal activities such as throwing motions 2. Acute-on-chronic injuries will reveal specific, mostly sportive activities in history, including acute pain, an audible popping sound leading to condition 2.
The clinical examination might reveal point tenderness at the insertion site of the anterior band of the ulnar collateral ligament at the sublime tubercle indicating valgus tress injury or medial epicondyle pain in skeletally immature patients indicating avulsion injury 2.
The specific pain might be reproduced with different valgus stress tests indicating valgus instability including the “milking manoeuvre” or “moving valgus stress test” 3,4.
Complications
Untreated valgus instability can lead to the following complications 2:
- early joint degeneration and osteoarthritis of the elbow
- cubital tunnel syndrome
Pathology
Valgus instability is the result of ulnar collateral ligament complex insufficiency especially of the anterior bundle, which develops from medial collateral ligament injuries.
Valgus stress causes a combination of tensile forces on the medial stabilising structures, compressive forces on the lateral compartment and posterior shear stress and is mitigated by the flexor-pronator muscle group 2-4. Injury happens if forces become too great and/or mitigation through the flexor-pronator muscle group fails.
In the throwing motion cycle, tensile forces on the medial side are highest during the late cocking and acceleration phase.
Aetiology
Valgus instability is most frequently a result of chronic overuse and less often develops in the setting of acute injuries (e.g. a fall on the outstretched hand) or acute-on-chronic injuries 1-3.
A less common cause of valgus instability is a failed treatment for acute elbow instability 2.
Radiographic features
Plain radiograph
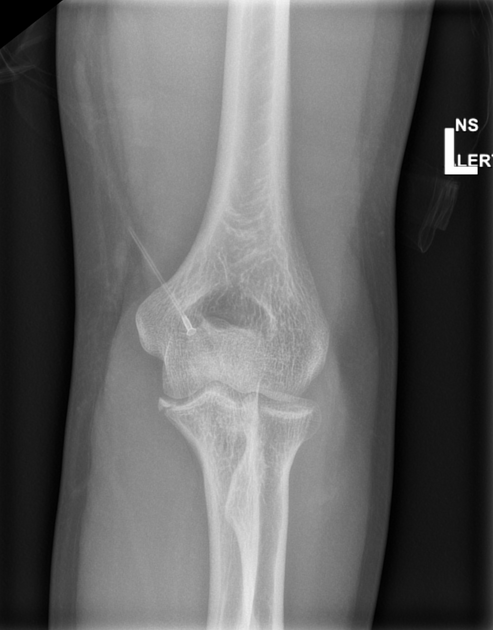
Plain standard anteroposterior and lateral views of the elbow might show ossifications of the medial epicondyle, loose bodies or periarticular osteophytes in a chronic setting or a medial epicondyle avulsion injury as well as concomitant radiocapitellar impression fractures in an acute injury 2-4. In addition, they might show an increased valgus carrying angle >20° 7.
In children, plain radiographs might demonstrate epiphysiolysis shown as widening of the apophysis 1.
Stress radiographs might show a medial joint line opening: >3 mm or a difference >0.5 mm towards the contralateral side is consistent with valgus instability 2,3
Ultrasound
Ultrasound might demonstrate ligament discontinuity with an anechoic fluid gap 3.
CT
CT can reveal associated bony lesions and fractures in the setting of an acute injury 1.
MRI
Full-thickness tears of the ulnar collateral ligament complex can be visualised on conventional MRI of the elbow as a discontinuity, redundancy or irregular pattern. Sprains and partial-thickness tears can be more difficult to demonstrate with increased T1 and T2 weighted imaging signals. Partial-thickness undersurface tears can appear as a “T-sign” at the lateral contour of the radioulnar joint 1-3,7.
Bone marrow oedema of the medial epicondylar apophysis can be also demonstrated on MR images indicating medial apophyseal stress injury 1.
MR/CT arthrography
MR or CT arthrography can nicely demonstrate partial-thickness undersurface tears of the anterior bundle of the medial collateral ligament complex with the “T-sign” on the ulnar-sided joint line of the ulnohumeral joint as a possible cause for valgus instability 1-3.
Radiology report
The radiological include a description of the following:
- bone marrow oedema within the medial epicondylar apophysis
- ulna collateral ligament complex sprains and/or tears with location and extent
- bony avulsions
- flexor-pronator mass injury
- radial head fractures
- signs of medial epicondylitis
Treatment and prognosis
Initial treatment is usually conservative and includes adequate rehabilitation after a resting period and pain control. Timely mobilisation is important and a dynamic brace with a stepwise increase to full extension might be a good option for reducing valgus stress and preventing stiffness at the same time. Strengthening exercises of the flexor-pronator muscle group, which helps to mitigate valgus forces as well as the extensor groups should be included in the rehabilitation program as well as special movement exercises (e.g. throwing mechanics) for athletes 2.
Operative management can be considered in athletes and high-demand patients in the setting of acute valgus instability and or after conservative treatment failure and includes direct repair, ligament reconstruction or hybrid techniques 1,4. Arthroscopy can be conducted beforehand to confirm the diagnosis and to address associated problems such as loose body removal and posteromedial impingement 2.
Differential diagnosis
Conditions that might mimic the imaging appearance of a valgus instability tear include:
- golfer’s elbow
- posteromedial rotatory instability
- posterolateral rotatory instability
- valgus extension overload syndrome



 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.