
Wilson disease, also known as hepatolenticular degeneration, is a multisystem disease due to abnormal accumulation of copper. It is characterised by early onset liver cirrhosis with CNS findings most frequently affecting the basal ganglia and midbrain.
This article aims to discuss the central nervous system manifestations of this condition. For a broad view on the condition, please refer to the main article on Wilson disease.
Clinical presentation
Neuropsychiatric manifestations of Wilson disease are protean. Common clinical features include dysarthria, dystonia, tremor, parkinsonism, choreoathetosis, ataxia, and gait anomalies. Kayser-Fleischer rings are also seen in nearly all patients with neurological manifestations of Wilson disease 1.
Radiographic features
Imaging features of Wilson disease can be variable, and depend on whether the disease is treated or untreated, and upon the degree of concurrent hepatic impairment. The most frequently affected neuroanatomical sites are the basal ganglia (especially putamen), followed by midbrain, pons, and thalamus 2,8. The distribution is typically bilateral and symmetric 4.
CT
In late stages, CT may demonstrate atrophic changes in the basal ganglia, cortical, and cerebellar regions 3:
non-enhanced: copper deposition does not increase density on CT
post-contrast: lesions do not enhance
MRI
MRI findings in Wilson disease can be highly variable 9.
-
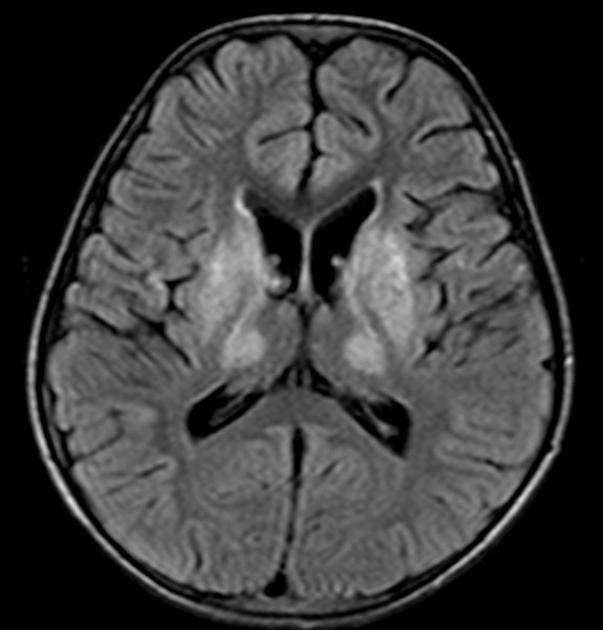
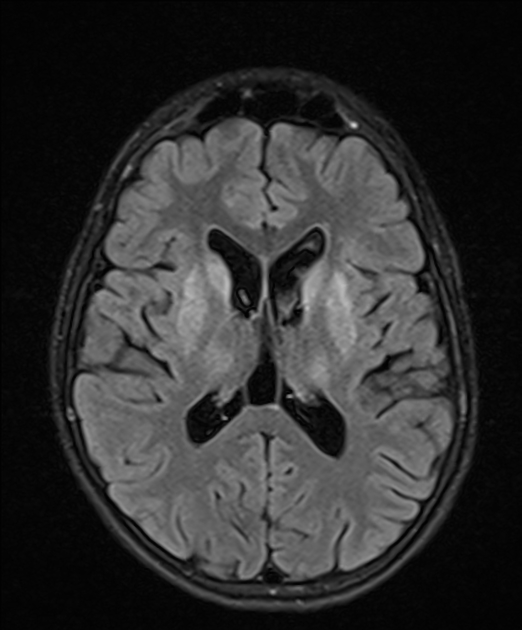
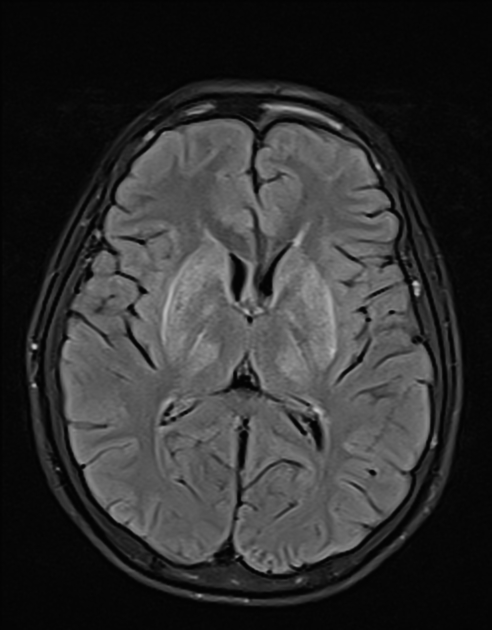
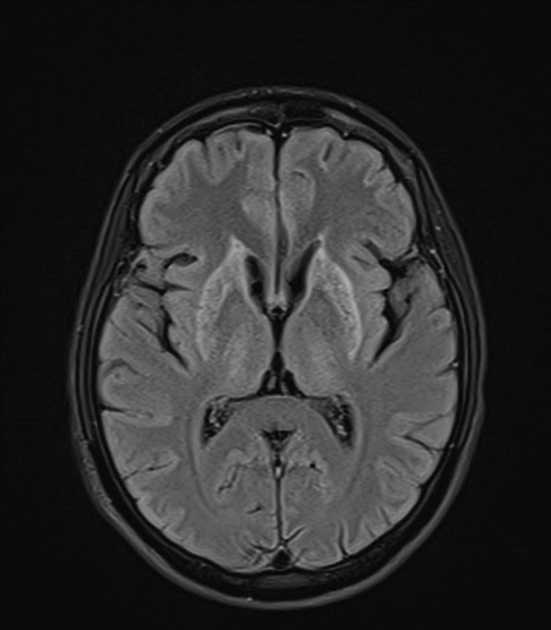
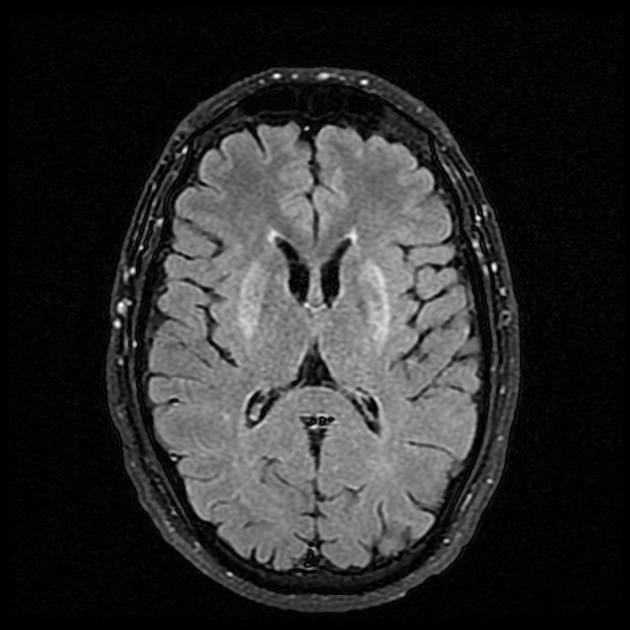
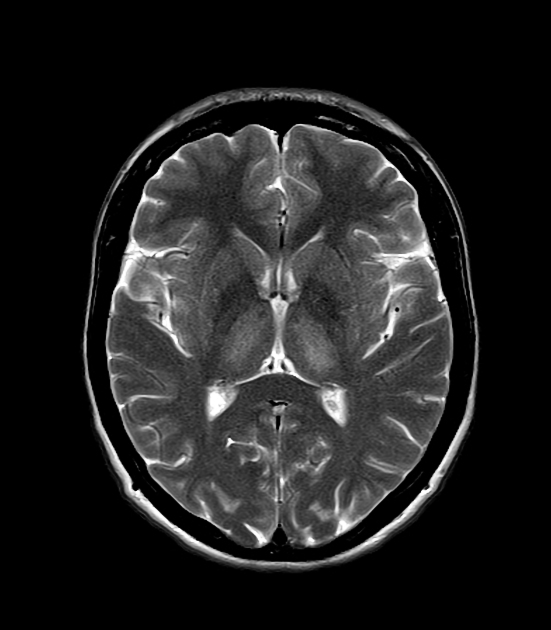
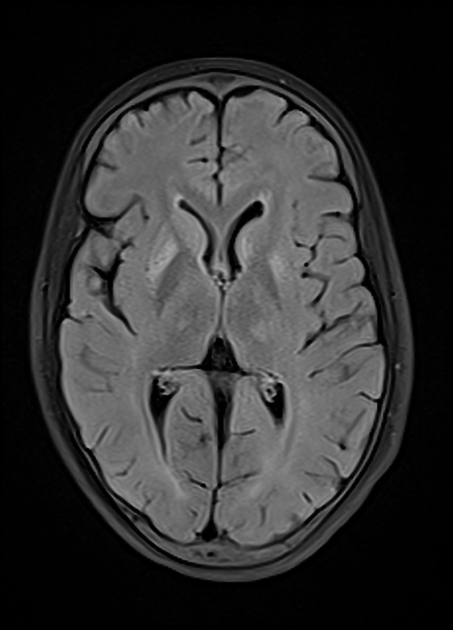
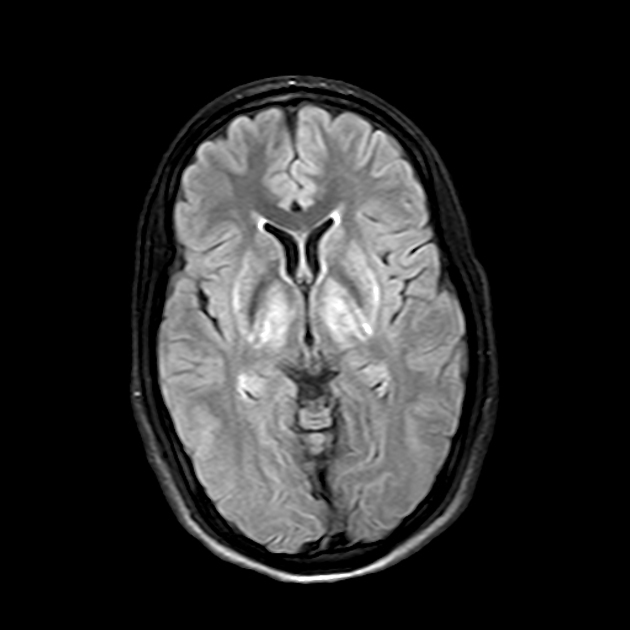
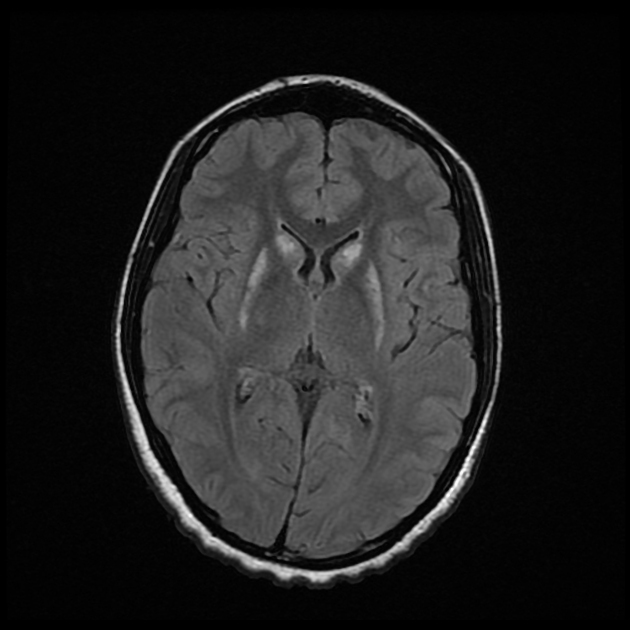
T2/FLAIR: multiple regions of the brain can potentially demonstrate abnormal signal change
abnormal hyperintensity in the putamina is the most common abnormality 4,8,9
additional areas of relatively common T2 signal abnormality can include the caudate nuclei, globus pallidi, ventrolateral thalami, and the deep gray nuclei in the midbrain 5,9
the pons and cerebellum are less commonly involved 9
in the cerebral hemispheres, symmetric, multifocal, leukoencephalopathy may uncommonly (~25%) be seen, with a frontal predominance 9
-
a number of radiological signs have been described on axial T2 imaging in Wilson disease, none of which are pathognomonic 6,9-11:
face of the giant panda sign: involvement of the midbrain tegmentum
face of the miniature (cub) panda sign: involvement of the pontine tegmentum
double panda sign: combination of the face of the giant panda sign and face of the miniature (cub) panda sign
bright claustrum sign: hyperintensity of the claustrum
split thalamus sign: within thalamic hyperintensity, a curvilinear hyperintensity is more prominently noted between medial and lateral groups of nuclei, seen to be 'splitting' the thalamus
whorl sign: concentric hyperintensities within the putamina
-
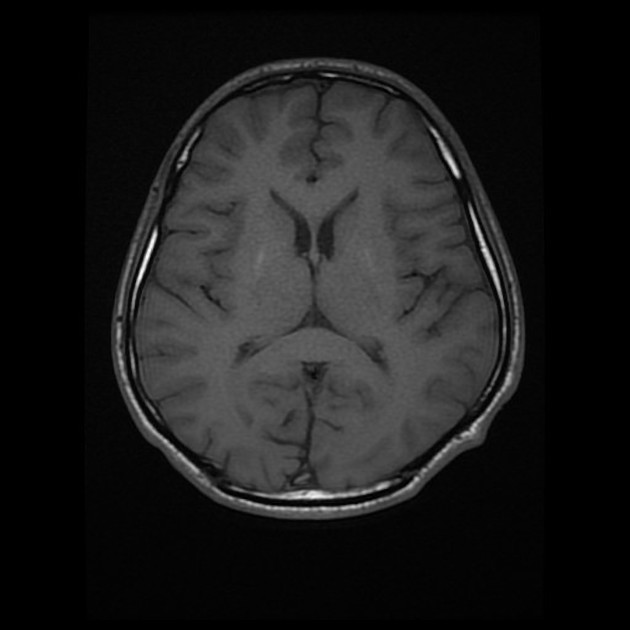
T1: signal abnormalities on T1-weighted images is variable, seemingly dependent on the degree of oedema and hepatic dysfunction 9
in patients presenting with neurologic manifestations, these areas show reduced T1 signal 2,9
in patients with severe hepatic dysfunction, these areas show increased T1 signal 2,4,9, especially in the globus pallidi, similar to that seen in acquired (non-Wilsonian) hepatocerebral degeneration attributed to manganese deposition 4
GRE/SWI: there may be blooming artifact in similar regions involved in abnormal T2 signal, including the putamina (most common), caudate nuclei, ventrolateral thalami, and dentate nuclei 9
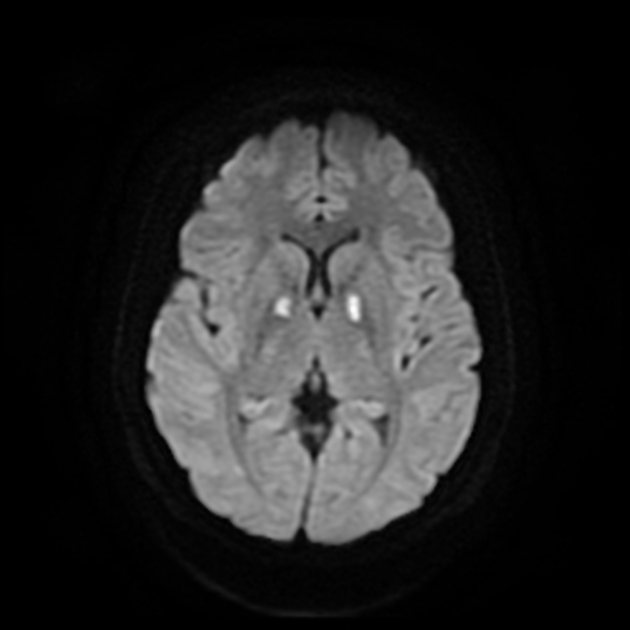
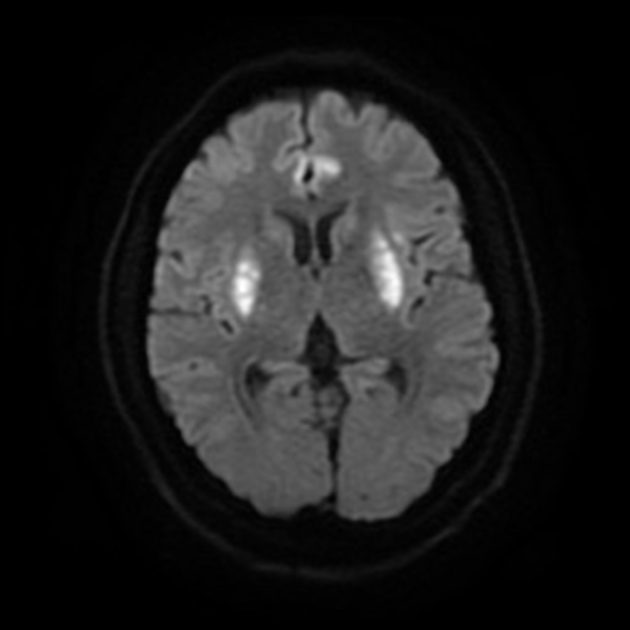
DWI/ADC: diffusion restriction may rarely be seen early in the course of the disease 7,9



 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.