
Presentation
Acute onset of left facial droop, left arm weakness, fixed rightward gaze, dysarthria. Background atrial flutter on DOAC.
Patient Data



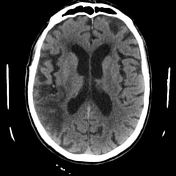
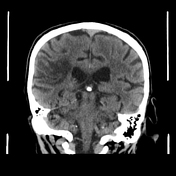
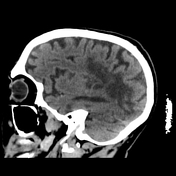
Non contrast CT brain demonstrates hyperdense vessel with in the right MCA, in the distal M2 superior division (with an "MCA dot sign"). There is corresponding complete occlusion on CT angiogram.
No signs of established infarct.

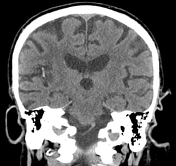

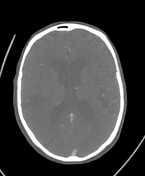
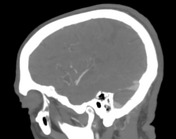
Acute/early subacute infarct in the right MCA territory with changes of cytotoxic edema: loss of grey-white matter differentiation, gyral swelling and local sulcal effacement.
Persistent hyperdense right M2 segment.
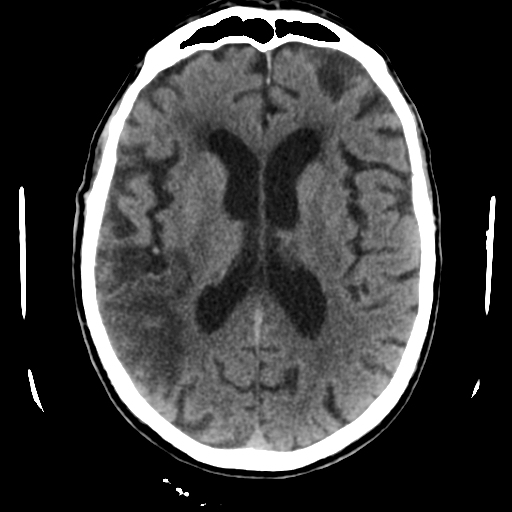
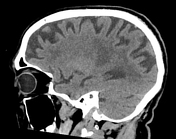
Expected progression of infarct in the right MCA territory. Improvement in the degree of edema with progressive density loss of the cortex and white matter, in keeping with encephalomalacia.
No hemorrhagic transformation.
Partial resolution of hyperdense M2 segment, suggesting ongoing thrombus resorption.
Case Discussion
This case nicely demonstrates the expected cerebral changes in acute ischemic infarct including the MCA dot sign.
The patient was not considered suitable for hyperacute intervention, due to current anticoagulation with apixaban and baseline functional level.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.