
Presentation
Abdominopelvic pain and progressive distention.
Patient Data


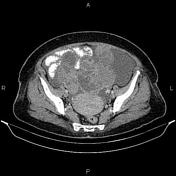
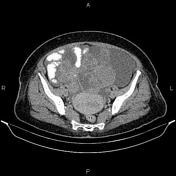


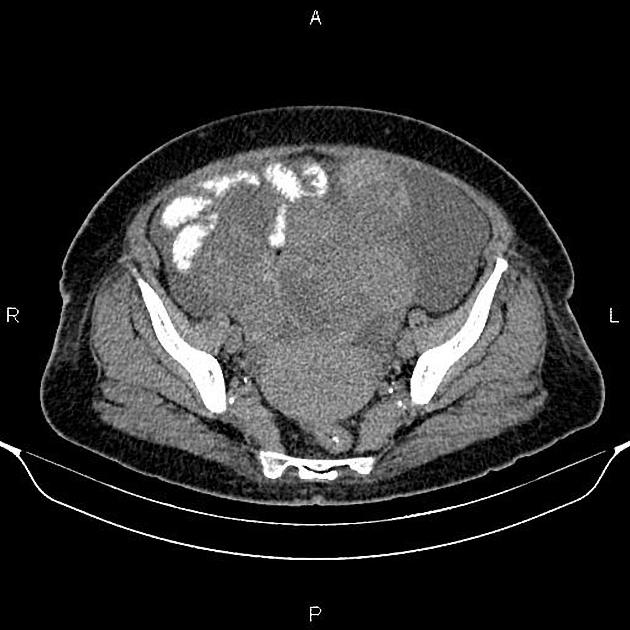
A 150×90 mm lobulated complex cystic solid mass is present at left adnexa.
A 105×62 mm similar mass is also noted at right adnexa. The ovaries could not be defined separate than mentioned masses. Endometrium is thickened.
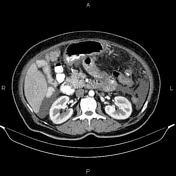
Moderate abdominopelvic ascites is present accompanied by omental thickening and multiple scattered soft tissue density masses inferring tumoral deposits.
A few lymphadenopathies are noted at para-aortic region with SAD less than 14 mm.
In imaged portions of lower thorax; several mediastinal and both hilar lymphadenopathies are seen.
Case Discussion
Bilateral ovarian masses; pathology proven ovarian serous cystadenocarcinoma with abdominopelvic ascites and tumoral deposits; mediastinal, hilar and para aortic lymphadenopathies.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.