
Presentation
Chronic headache for 2 years, which become worsened for the past 1 day, together with increased intracranial pressure symptoms.
Patient Data



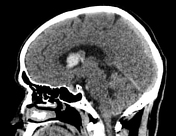

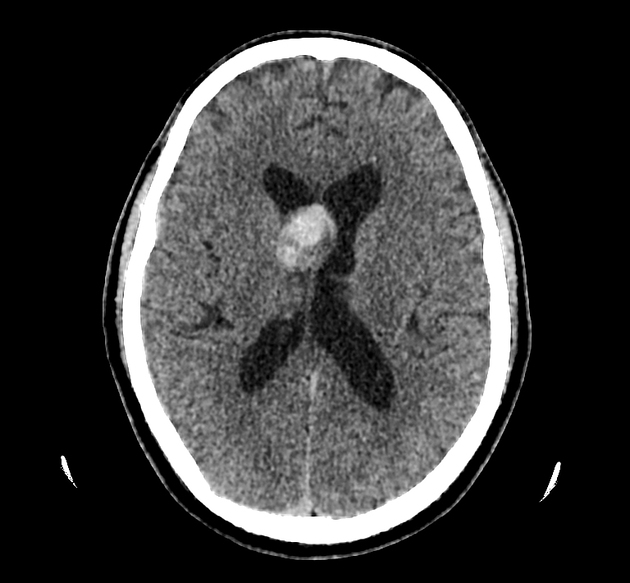
A well circumscribed hyperdense lesion located at right lateral ventricle(near to the foramen of Monro) which appears to be attached to the septum pellucidum. It has attenuation number of 65 to 70 HU, likely to represent hemorrhagic component. No obvious hyperdense layering seen within the right lateral ventricle to suggest intraventricular hemorrhage. However, all ventricles appear dilated in keeping with hydrocephalus. Post contrast administration, no significant enhancement.
No other focal enhancing brain parenchymal lesion.
No significant midline shift.
Case Discussion
CT features are suggestive of central neurocytoma with evidence of intratumoral bleed and hydrocephalus which contribute to the patient’s symptoms (headache and vomiting).
Central neurocytoma is rare central nervous system WHO type 2 intraventricular tumor. The incidence of spontaneous hemorrhage as presentation is exquisitely rare.1
According to retrospective study by Wang et al2, the incidence of central neurocytoma hemorrhage was 5 of 63 cases (7.9%).
The definitive treatment is total resection of the tumor.
The patient underwent emergency craniotomy and excision of the mass which confirmed the diagnosis of bleeding central neurocytoma.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.