
Presentation
Insidious onset of severe right shoulder pain, somewhat acute.
Patient Data




There is extensive calcification within the subacromial space which is homogenously dense and amorphous in shape. The humeral head is displaced inferolaterally with a widened glenohumeral joint space and acromiohumeral distance, likely due to effusion.
It is unclear whether this calcification is intratendinous with a large underlying gelnohumeral joint effusion, or in the subacromial bursa above the supraspinatus inciting an intense inflammatory reaction and bursitis, subluxating the humeral head.
Feeling significantly better, but still with some pain, the patient returns for an MRI a couple weeks later to assess for rotator cuff pathology and internal derangement.
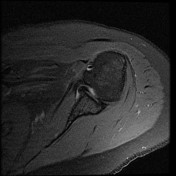

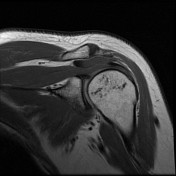
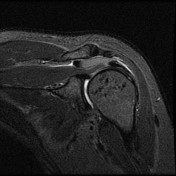

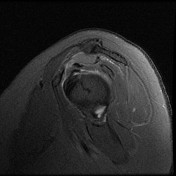
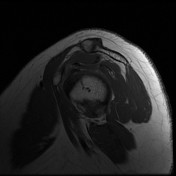
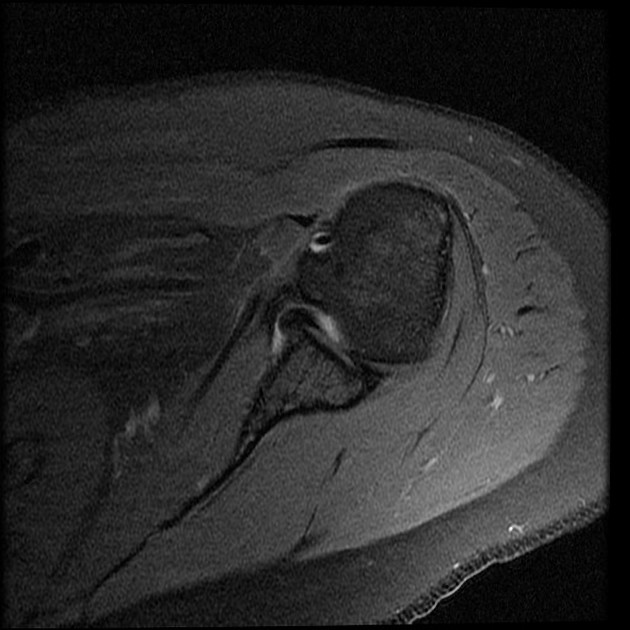
The subacromial/subdeltoid bursa is distended with a T1 and STIR isointense fluid with a gravity dependent T1/STIR hypointense layer which corresponds to the area of calcification in the comparison radiographic study, indicating milk of calcium. This collection causes mild mass effect on the underlying rotator myotendinous junction. No discrete rotator cuff tear or calcification is identified, however near the supraspinatus insertion there is some architectural distortion of the tendon fibers near their insertion on the footplate. Deep to this area within the greater tuberosity there are multiple T1/T2 hyptointense foci which appear to extend out from the footplate. There is decreased bulk of the supraspinatus muscle suggesting mild atrophy.
Incidentally, a redundant fold of the middle glenohumeral ligament and subscapularis is seen in and along the anterior glenohumeral joint due to internal rotation of the humerus at the time of scanning.
Case Discussion
Calcific bursitis may occur in isolation or in association with calcium hydroxyapatite deposits in a tendon/myotendinous junction (calcific tendinitis). In the latter scenario, which some might argue is always the scenario, the calcium hydroxyapatite crystals erode into an adjacent bursa. In the bursa, an intense inflammatory reaction is typically incited which may lead to liquefaction (into milk of calcium) of the calcific mass, as demonstrated in this case.
Uniquely however, in this case it is difficult to make a convincing argument for the rotator cuff damage that would be expected to be seen with previous calcific tendinitis. Given the odd pattern of presumable calcifications in the greater tuberosity (low on T1 & T2, however occult on the radiographs) this was likely the case, as the crystals can migrate into the humerus just as they can into the bursa.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.