
Presentation
Headache
Patient Data


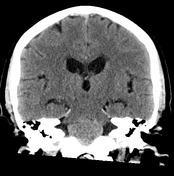
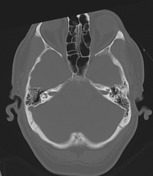
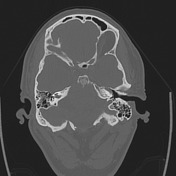
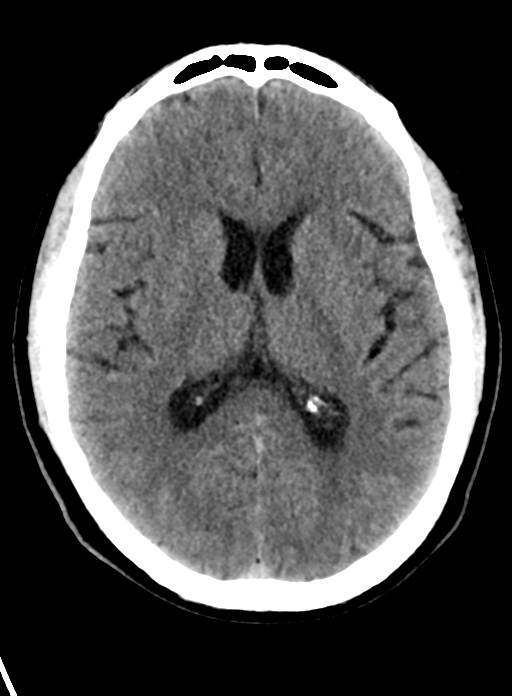
Lobulated extra-axial mass centered on the pre-pontine and pre-medullary cisterns. The mass is hyperdense with a punctate focus of internal calcification posterosuperiorly. There is compression on the adjacent brainstem and the fourth ventricle, better appreciated on recent MRI, with bilateral temporal horn dilatation which is unchanged. There is evidence of associated clival erosion with destruction of cortical bone predominantly to the right of the midline. Mild periventricular white matter and left frontal hypodensity are unchanged. No further abnormality is seen.
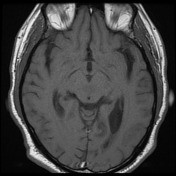
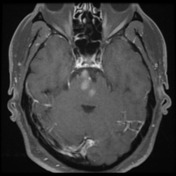
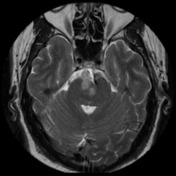
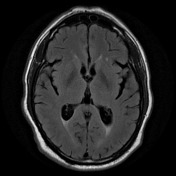
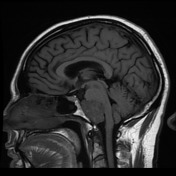
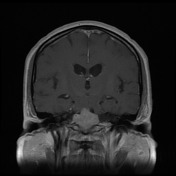
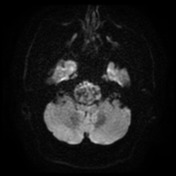
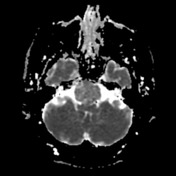
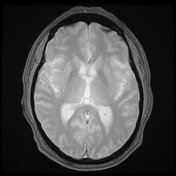

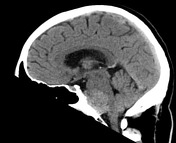
A multilobulated extra-axial midline enhancing mass lesion contacting the clivus, indenting the brainstem and obliterating the pontomedullary cistern. The lesion is moderately heterogeneous, mainly T1 hypointense to brain, with some small foci of T1 hyperintensity and scattered foci of susceptibility. Although the lesion is predominantly T2 hyperintense, it is of lower signal to the adjacent CSF. Despite the indentations of the brainstem "thumb sign", there is no brainstem edema. No dural tail. The basilar artery is displaced to the left and posteriorly, partially encased by the tumor. Within the limits of MRI, there is possible minor erosion of the clivus. The 4th ventricle is distorted inferiorly. The temporal horns remain dilated, with periventricular FLAIR hyperintensity.
Conclusion: The midline solidly enhancing extra-axial mass lesion in the pontomedullary cistern with internal foci of susceptibility. It is more probably a chordoma than meningioma (with calcification and/or hemorrhage).
Case Discussion
The patient went on to have surgery.
Histology
MICROSCOPIC DESCRIPTION: The sections show an epithelioid tumor, forming cords and nests, embedded in prominently myxomatous stroma. The tumor invades into bony trabeculae in the medulla. The tumor cells have mildly enlarged and hyperchromatic ovoid nuclei, small nucleoli and moderate amounts of eosinophilic cytoplasm. Scattered physaliferous cells are seen and they show cytoplasmic vacuolation. Lymphovascular invasion is absent. The tumor cells are CAM5.2 positive. The Ki-67 index is about 2%. S-100 and M2A are negative. The features are those of chordoma.
FINAL DIAGNOSIS: Chordoma.
Discussion
Although most chordomas have more bony destruction than this lesion, the direct posterior direction of growth and relatively high T2 signal are common features.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.