
Presentation
Chronic abdominal pain. Colonoscopy showed thickening of the mid rectum and a submucosal hemorrhagic mass with suspicion of malignancy.
Patient Data


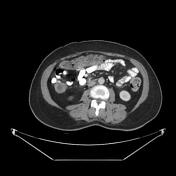



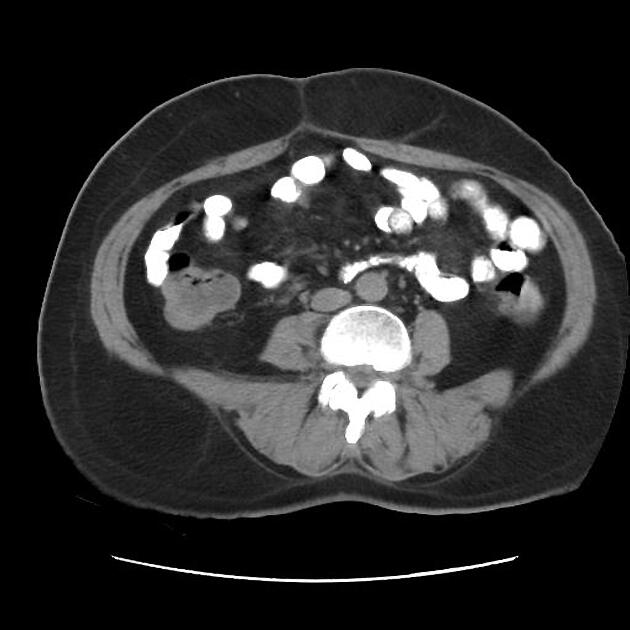
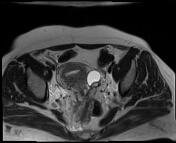
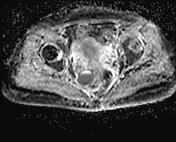
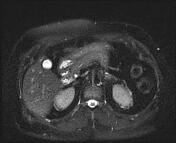
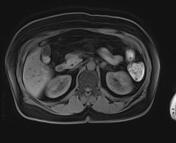
asymmetrical wall thickening of the mid to lower rectum is associated with mesorectal fascia fat stranding and cystic lesion measuring about 28 x 35 mm along with the right side of the rectum at 9 o'clock within the mesorectal fascia
few mesorectal fascia lymph nodes with a maximum SAD of 6 mm
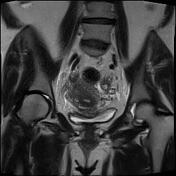
thickening of the right-sided uterosacral ligament
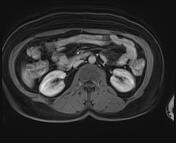
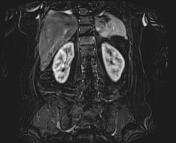
left adnexa hypodense cystic lesion measuring about 33 mm
a 10 mm hypodense lesion along with the left adrenal gland medial limb
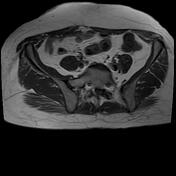


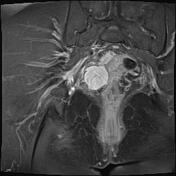
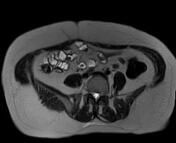

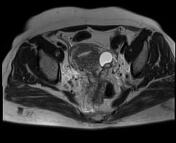
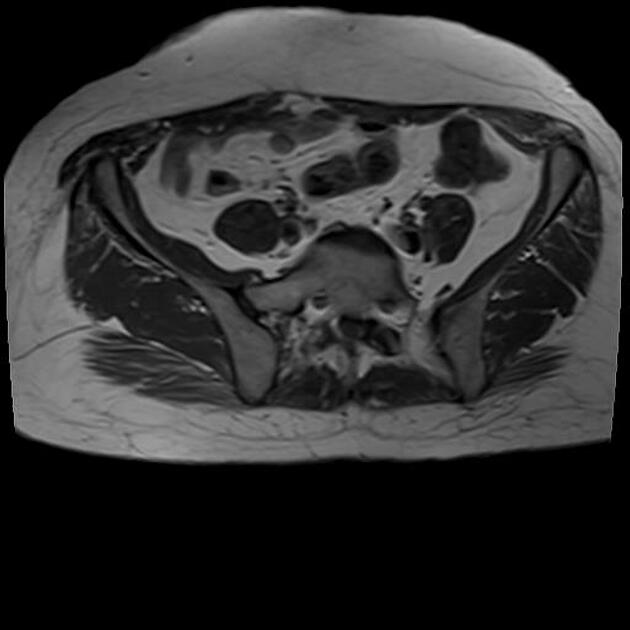
two abnormal signals (low to intermediate on T1 and high on T2) cystic lesions measuring about 28 x 33 mm and 10 x 12 mm along with left adnexa with a thin rim of post-contrast enhancements
right ovary measuring about 17 x 27 mm
adhesion of ovaries to the serosal surface of the uterus on each side
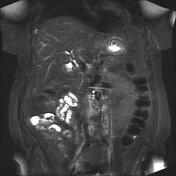
a 28 x 36 mm cystic lesion of T1 fat sat hyperintensity giving T2 shading appearance with a thin peripheral enhancement located in the mesorectal fascia at the level of mid rectum 9 o'clock with adhesion to the muscularis propria
left-sided hydrosalpinx with a maximum fallopian tube width measuring about 10 mm
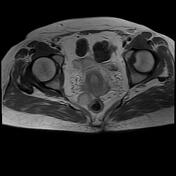
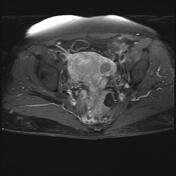
marked thickening of bilateral uterosacral ligaments more obviously on the right side in the background of the diffuse spread of multiple endometriotic nodules throughout the USLs
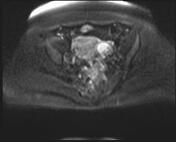
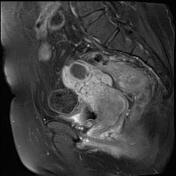
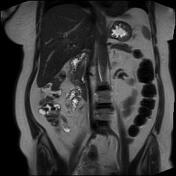
obliteration of the culdesac space because of numerous endometriotic nodules (diffuse endometriosis) with direct invastion to the serosal surface of the rectum, traversing the mesorectal fascia and muscularis properia and producing a submucusal masslike lesion measuring about 10 x 20 mm along with mid to lower rectum which causing to wall thickening and irregularity at the mid to anterior aspects of midrectum
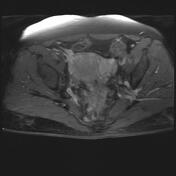
advanced desmoplastic reactiobn and subsecquent enhancements are seen in contact with aformentioned diffuse endometriosis of recto-uterine area and next to the the endometrima cyst in right sided mesorectal area resulting in external deviation of the rectum
uterus showed heterogeneous signal intensity with post contrast heterogenous enhancements
Case Discussion
deep extensive pelvic endometriosis (Cullen's syndrome) with infiltration of the posterior fornix, torus uterinus, mesorectal fascia, and rectal wall muscularis properia with submucosal infiltration that mimicking a rectal mass
advanced desmoplastic reactions along with the mid to lower rectum especially the right para midline of the rectum associated with the thickening of uterosacral ligaments
endometrioma cysts along with left adnexa and within mesorectal fascia at 9 o'clock
diffuse endometriosis implants display T1 high signal intensity on T1WI sequences in col de sac space and mesoraectal fascia


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.