
Presentation
Painless, rapidly growing lump in the left breast, discovered two months before the consultation. She had no history of trauma.
Patient Data

On examination, there was a 10 x 6 cm firm mass in the upper quadrants of the left breast. The mass was mobile but appeared to be fixed to the skin which was stretched and discoloured. No edema or "peau d'orange" changes. The nipple was not retracted.

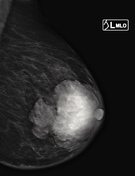
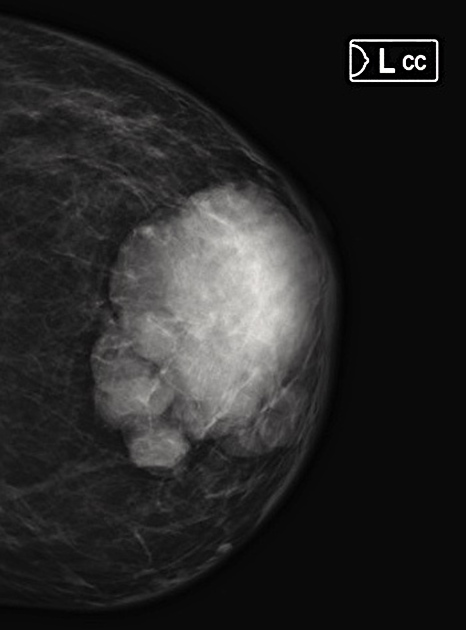
Mammographic imaging of the left breast shows a high-density dishomogenous lobulated mass, with well-circumscribed margins and no microcalcifications
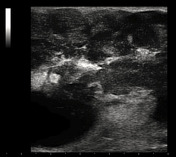
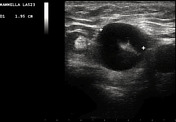
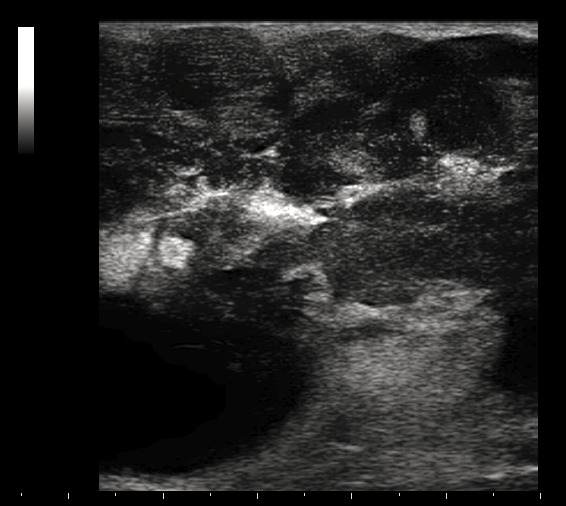
Ultrasonography shows a heterogeneous, irregular, mixed hyper- and hypo-echoic mass with a lobulated margin. The overlying skin appears normal.
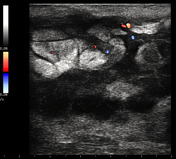
Color Doppler imaging shows internal vascularity; i.e. vessels are detected within the mass.
The axillary lymph nodes were enlarged, with the largest measuring 2 cm in diameter and showed a cortical thickness greater than 3 mm.
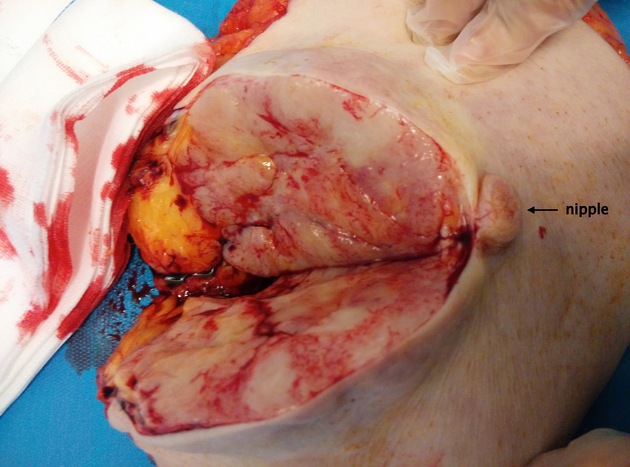
A radical mastectomy and a complete axillary dissection were performed. The section of the specimen shows the lobulated pattern of the mass.
Case Discussion
The pathologic diagnosis was a primary non-Hodgkin's lymphoma of the breast and of the 27 axillary lymph nodes removed (diffuse large B-cell lymphoma or DLBCL).
Key learning points:
- primary lymphomas represent 0.5% of all breast malignancies
- the most frequent subtype is diffuse large B-cell non-Hodgkin's lymphoma (NHL) accounting for approximately 25% of NHL cases, followed by follicular lymphoma
- they have a typical bimodal distribution of age-specific incidence rates with two peaks in the 4th and the 7th decades of life
- the pushing margins of the lesion (see clinical, mammographic, and pathological pictures) are related to its rapid grow


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.