
Dorsal dermal sinus - with spinal inclusion cyst and tethered cord
Presentation
Lumbar discharge.
Patient Data







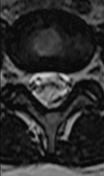

Intradural extramedullary lobulated mass nestled within the cauda equina at the L4-L5 intervertebral level showed slightly higher signal intensity than CSF on T1, hypersignal on T2, high signal on DWI with true diffusion restriction on the ADC map without contrast enhancement likely in keeping with an intraspinal inclusion cyst (most likely an epidermoid cyst). The mass displaces the cauda equina nerves peripherally.
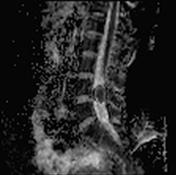
Abnormal conus elongation with low termination at the L3-L4 intervertebral level along with slightly thickened filum terminale which seems to be attached to the aforementioned soft tissue mass (tethered cord).
Subcuaneous tract extending from the skin to the spinal canal at the level of S2 vertebra showing hyposignal on T1, hypersignal on T2 with parietal contrast enhancement after gadolinium administration (dermal sinus).
Case Discussion
Spinal epidermoid cyst may be congenital, arising from epidermal rests or dermal sinus, or acquired (iatrogenic) following implantation of viable epidermal elements after lumbar puncture or surgery. A spinal epidermoid cyst is associated with dermal sinus in 20% of cases.
The main differential diagnosis is spinal dermoid cyst, which is less likely to show diffusion restriction than an epidermoid cyst and may contain interspersed fat signal intensity.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.