
Presentation
Incidental hypervascular liver lesion found on chest CT.
Patient Data

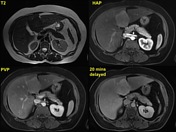

Non-cirrhotic liver. A well circumscribed lobulated mass is seen in liver segment IVb. This lesion is minimally hypointense on both the T1 and T2 weighted images and does not contain fat. A subtle central T2 hyperintense scar is evident. Background of intracellular hepatic steatosis with relative loss of signal on the out-of-phase sequence.
Following administration of Primovist (GD EOB DTPA) T1 FS images showed avid enhancement during the arterial phase followed by iso/slight hyperintensity during the portal venous phase. The 20 minutes delayed image demonstrate persistent intralesional hyperintensity and this confirms the diagnosis of FNH.
Case Discussion
Hepatobiliary agents are the preferred choice of contrast agent in evaluation of hypervascular liver lesion especially when FNH is suspected. In Australia Primovist (GD EOB DTPA) and in North America the equivalent Eovist are most widely used. Both are ionic agent with 50% renal and 50% bile excretion. The delayed hepatocyte phase commence 10 minutes post injection and data can be acquired at 20 mins with a potential window of 120 mins.
MultiHance (GD BOPTA) is another hepatobiliary agent available however due to its elimination profile, 97% renal and 3% bile, a longer delayed period of 1-2 hours is required for imaging acquisition. Thus this is a less popular agent of choice for evaluation of FNH.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.