
Presentation
Staging CT for gastric lesion found on gastroscopy.
Patient Data
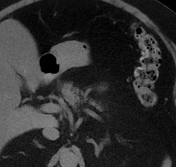



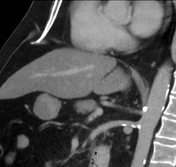
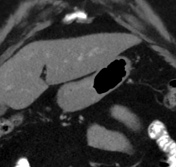
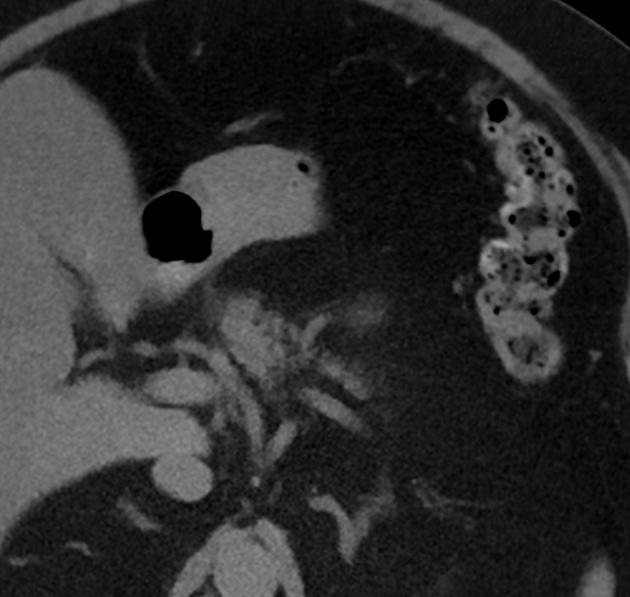
There is a hypodense mass in the gastric antrum located in the anterior gastric wall/great curvature and in keeping with the gastroscopy findings. No nodal or distant metastatic disease to the abdomen and pelvis.
Macroscopy: Labelled "Distal gastrectomy". A partial gastrectomy 93 mm proximal to distal and 52 mm in diameter, stapled proximally and distally (staples trimmed and proximal margin inked green, distal margin inked blue). Within the distal portion of the specimen, located within the submucosa, is a firm solid pale tan mass 33 x 29 x 13 mm. The mass is 11 mm from the trimmed distal margin and greater than 40 mm to the proximal margin. The tumour macroscopically abuts but does not macroscopically invade the muscularis propria and immediately underlies the intact mucosa. A small amount of attached fat is present on the serosal surface, up to 4 mm, no lymph nodes identified.
Microscopy: The sections show a well circumscribed but an unencapsulated tumour within the submucosa of the antrum comprising thick intersecting fascicles of spindled cells with elongate nuclei and abundant eosinophilic cytoplasm. Scattered cells show nuclear atypia comprising nuclear enlargement and hyperchromasia with nuclear membrane irregularities. No significant mitotic activity is seen and there is no necrosis. The atypia is consistent with symplastic change. The lesion is clear of all excision margins. Using immunohistochemical stains, the tumour cells are positive for desmin and negative for CD117, CD34 and S100.
The gastric mucosa shows severe chronic inflammation with numerous plasma cells and occasional secondary lymphoid follicles present within the lamina propria. Significant active inflammation is not seen. Scattered Helicobacter-type organisms present within surface mucin.
Opinion: Distal gastrectomy specimen: Leiomyoma, size 33 mm within the antral submucosa, clear of excision margins. Chronic Helicobacter pylori-associated gastritis.
Case Discussion
External gastroscopy biopsy had shown features of leiomyoma, but there was not enough tissue for an accurate diagnosis. The patient underwent partial gastrectomy that confirmed a benign gastric leiomyoma.
This is case not for radiology diagnosis, as the lesion can be easily missed on CT without knowing about its existence.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.