
Presentation
Painful right eye swelling with reduced visual acuity for 5 days.
Patient Data
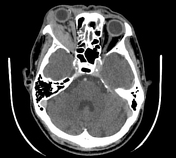

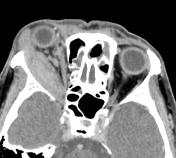

significant right eye proptosis
the right lateral rectus and medial rectus extraocular muscles are diffusely enlarged including their tendinous insertion. The right lateral rectus muscle is more severely affected
at the orbital apex, there is moderate obliteration of the perineural fat surrounding the optic nerve complex
smudging fat streakiness at intraconal and extraconal compartments of the right orbit
mild right preseptal soft tissue thickening
the right lacrimal gland is moderately enlarged and showing homogenous enhancement
the right superior ophthalmic vein and right cavernous sinuses are well opacified and not enlarged
left orbit is normal
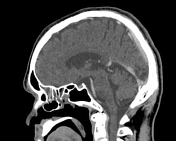
mucosal thickening at both ethmoidal and left frontal sinus. No bone erosion, especially the right lamina papyracea. No subperiosteal abscess.


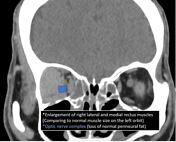
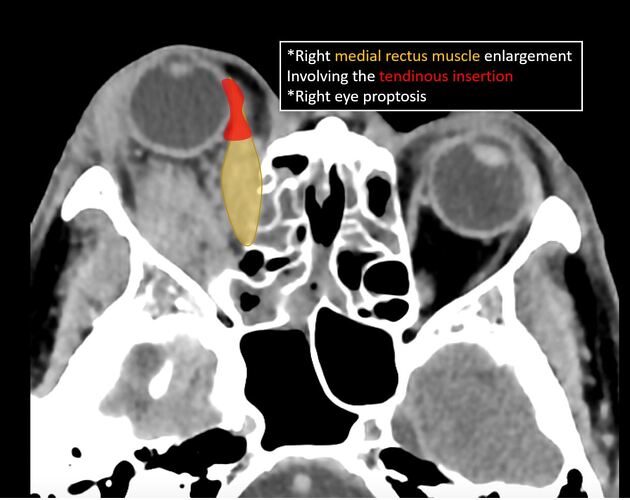
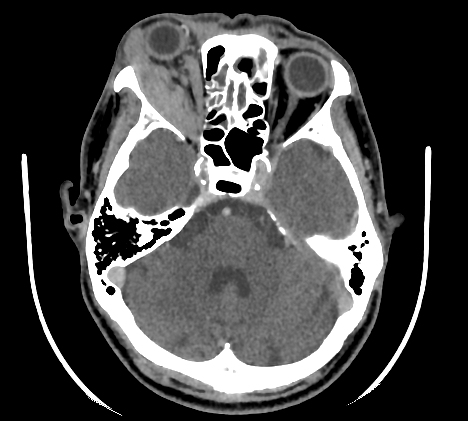
annotated images showed the enlargement of right lateral and medial rectus muscles with involvement of tendinous insertion
perineural fat surrounding the right optic nerve complex is obliterated at the orbital apex
cavernous sinuses are not enlarged
Case Discussion
Idiopathic orbital inflammation of the orbit can basically involve any part of the orbit (including lacrimal glands, orbital content, and extraocular muscles) but usually affects the extraocular muscles. The patient was treated with corticosteroids. On follow-up, patient's symptoms and signs resolved.
The most important differential diagnosis to be considered is thyroid orbitopathy, which itself has involvement of tendinous insertions of muscles and involves the muscles in the sequence of I'M SLOw (inferior rectus would be affected first before the medial rectus and lateral rectus). Therefore, in our case, the involvement of the tendinous insertion, unilaterality as well as the lateral rectus is much more affected made the diagnosis of thyroid eye disease unlikely.
The obliteration of the perineural fat at the orbital apex raises the suspicion of orbital apex crowding syndrome which may lead to optic neuropathy. This imaging finding should be alerted to the referring ophthalmologist.
A few clinical and imaging points to consider for any case with enlargement of extraocular muscles:
involvement of the tendinous insertion to the orbit
any enlargement of superior ophthalmic vein or cavernous sinus, which can raise the suspicion of carotico-cavernous fistula or Tolosa Hunt syndrome
unilaterilty vs bilaterality
which particular extraocular muscles are involved
painful vs painless eyes


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.