
Presentation
Past medical history of COPD, a neurocutaneous syndrome, and bipolar disease undergoes an ultrasound as part of a workup for seizures. US (not available) revealed a mass centered in the left retroperitoneum. A CT scan was performed for further workup.
Patient Data


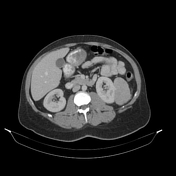
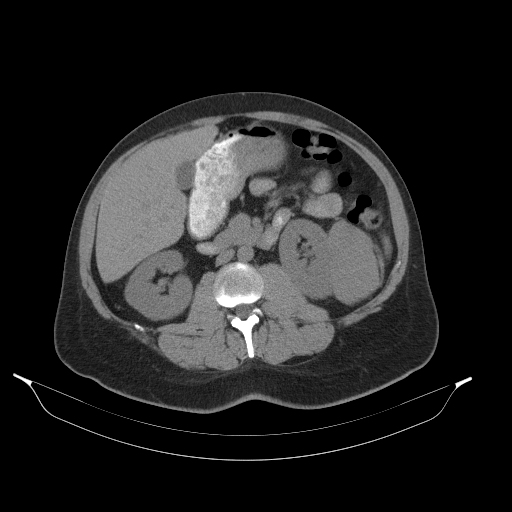
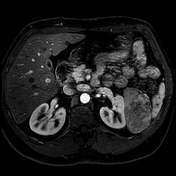
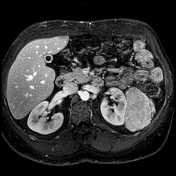
Non-contrast CT images of the abdomen and pelvis demonstrate a fairly homogenous and mildly hyperattenuating (HU 41) mass centered in the left retroperitoneum with at least an abutment of both the left kidney and spleen.
Post-contrast CT images demonstrate the mass to be enhancing homogeneously, to a lesser degree than adjacent renal parenchyma. No fat or calcification was identified within the mass.
Left renal small stones are also noted.
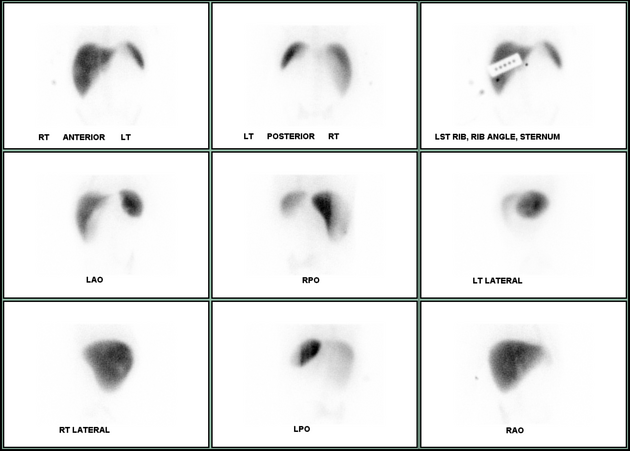
A sulfur colloid scan demonstrates no uptake of radiotracer associated with the mass.
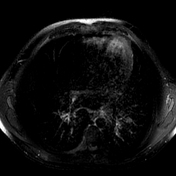
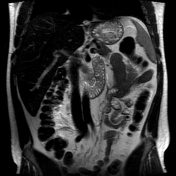
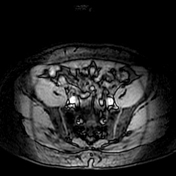


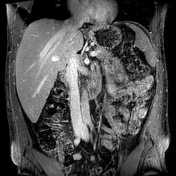
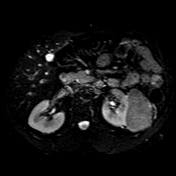
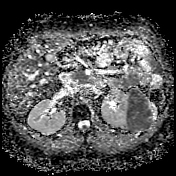
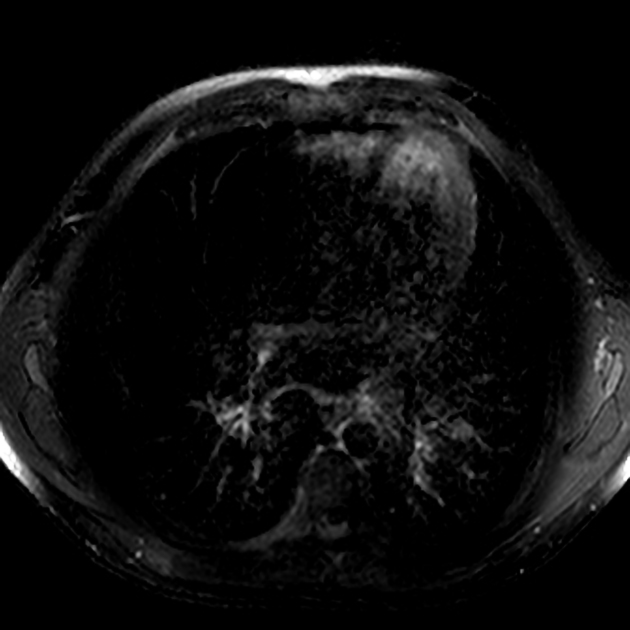
MRI demonstrates a 7.5cm mass centered in the left retroperitoneum with homogeneous hypointense signal on conventional T2-WI, isointense signal on FS T2-WI, isointense signal on T1-WI, and no intracellular or macroscopic fat. Post-contrast images demonstrate minimal intervening renal parenchyma along the medial margin of the mass, as well as relatively homogenous and continuous enhancement, with relative washout on more delayed images and no significantly prominent arterial phase hyperenhancement. Delayed post-contrast images demonstrate enhancement of small vessels within the mass. The mass shows diffusion restriction on DWI/ADC images reflecting hypercellularity.
Case Discussion
The patient has a history of tuberous sclerosis, which portrays an increased risk of developing benign or malignant renal masses. The mass on CT was suspected to potentially represent an accessory spleen or indeterminate tumor. A sulfur colloid scan revealed that the mass did not contain splenic tissue. An MRI was ultimately recommended for further characterization. The patient underwent resection of the mass which revealed a lipid-poor angiomyolipoma arising from the renal parenchyma, a not uncommon finding in patients with TS.
Key points:
Lipid-poor AMLs are difficult to distinguish from RCC. The lack of calcification, the relatively homogenous hyperattenuation (>40 HU) on non-contrast CT, and homogenous and continuous enhancement favor lipid-poor AML.
RCC typically displays more prominent wash-in and wash-out characteristics than lipid-poor AML.
RCC are typically hyperintense on T2-WI, whereas lipid-poor AML are hypointense.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.