
Presentation
Left ear pain and fever not improving on antibiotics.
Patient Data
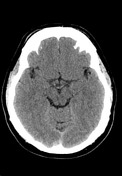

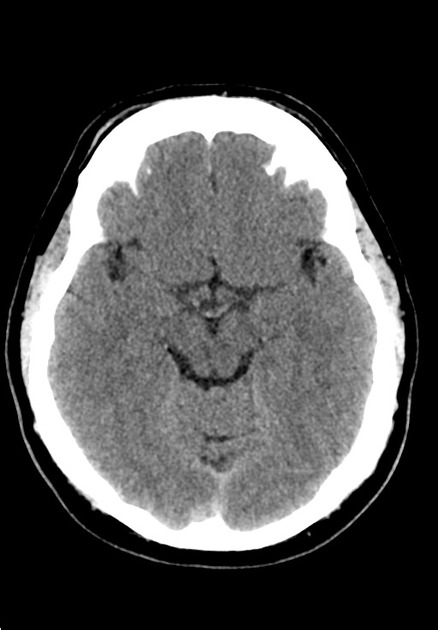
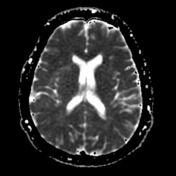
No intra- or extra-axial collection or hemorrhage demonstrated. No focal abnormality. Grey-white differentiation is preserved. Ventricular size, sulcal pattern and basal cisterns all appear normal. Dural venous sinuses are normal density.
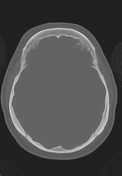
Opacification of the left middle ear cleft and left mastoid air cells. No bony destruction or ossicular disruption. Soft tissue thickening of the external acoustic canal. The fossa of Rosenmuller is unremarkable.
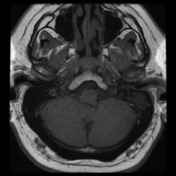
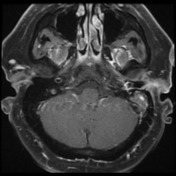

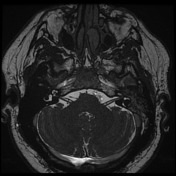
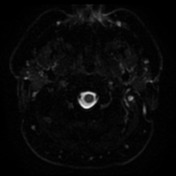

Left middle ear cleft and mastoid are fluid-filled with associated peripheral post contrast-enhancement. There is enhancing edema also extending beyond the mastoid tip. No widespread diffusion restriction, although there may be a focus in the most inferior mastoid air cell.
Case Discussion
The presence of fluid in the mastoid air cells does not automatically make the diagnosis of mastoiditis. If there is absence of bony destruction on CT (or other complications), the diagnosis is impossible to make. On MRI, the presence of fluid in the mastoid air cells should be accompanied by mucosal enhancement and/or diffusion restriction is required. The presence of extramastoid change (in this case the soft tissue enhancement at the tip of the mastoid process) is also a helpful adjunct in making the diagnosis.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.