
Presentation
Headaches. Previous history of prophylactic cranial irradiation (DXT) for acute lymphoblastic leukaemia (ALL) in childhood.
Patient Data



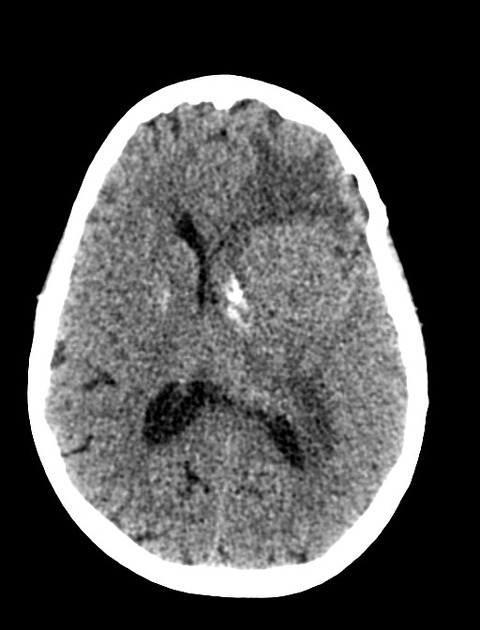
Multiple high-density lesions in an extra-axial location are identified on both sides of the brain, the biggest ones on the left. They have a vivid contrast enhancement and, some of them, necrotic hypoattenuating central areas. The largest arises from the left sphenoid wing in the left middle cranial fossa and promotes mass effect with compression over the left lateral ventricle and mild midline shift to the right, regional oedema, as well as left transtentorial herniation downward.
Conclusion: The lesions are in keeping with multiple meningiomas which are probably secondary to radiotherapy treatment in childhood.
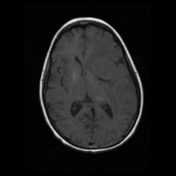

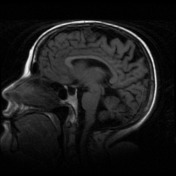

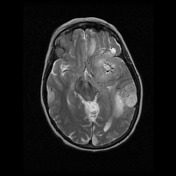
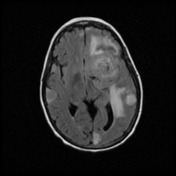
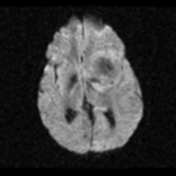
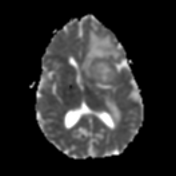
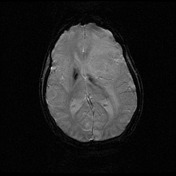
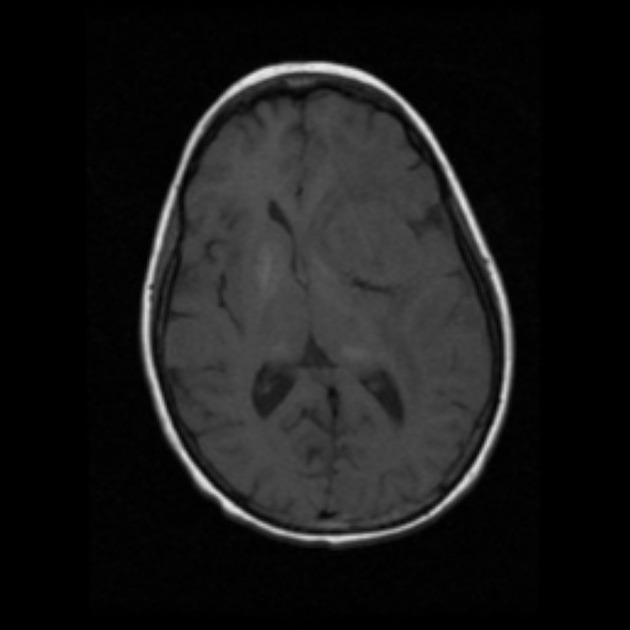
The multiple extra-axial lesions are again demonstrated, showing iso-signal on T1 and high signal on T2 compared to the adjacent brain, keeping the vivid contrast enhancement and, some of them, with a necrotic hypoattenuating central area. The largest one arises from the left sphenoid wing in the left middle cranial fossa and promotes mass effect with compression over the left lateral ventricle and mild midline shift to the right, regional oedema, as well as left transtentorial herniation downward.
The second largest mass, arising from the parietal bone on the left demonstrates increased T2 signal and facilitated diffusion on ADC.
Conclusion: The lesions are in keeping with multiple meningiomas which are probably secondary to prior radiotherapy treatment.
Case Discussion
This patient had total body radiation for acute lymphocytic leukaemia when a child.
These are radiation-induced meningiomas, which are more frequently multiple and have a very long latency.
The patient went on to have resection of the two largest left sided tumours.
Histology
The paraffin sections show a variably hypercellular dural-based tumour. Tumour cells are a mixture of epithelioid and spindle morphology and are arranged in diffuse sheets and loose fasciculi. In many areas, a chordoid appearance is also noted with solid aggregates and cords of epithelioid tumour cells dispersed within a myxomatous stroma.
Tumour cells show moderate nuclear pleomorphism and an occasional mitotic figure is identified (1/20 HPF). No areas of necrosis are seen. There is no brain invasion.
Immunohistochemistry shows strong nuclear staining in tumour cells for progesterone receptor (PgR) and strong membrane staining for epithelial membrane antigen (EMA). There is also moderate staining for bcl-2 and patchy moderate staining for smooth muscle actin (SMA). No staining for CD34, ALK-1, desmin or pancytokeratin AE1/AE3 is seen in tumour cells.
DIAGNOSIS: Chordoid meningioma (WHO grade II).


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.