Presentation
Intermittent pelvic pain, persistent hematuria, and left flank pain.
Patient Data
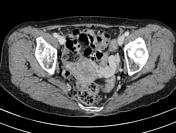




Multiple venous varicosities were seen in bilateral para uterine/parametrial regions, more dilated on the left side. The largest diameter of the left para-uterine vein measures 1.0cm.
Bilateral ovarian veins are enlarged, measuring up to 0.9cm. There are duplications of bilateral ovarian veins which are the common normal variants.
Left ovarian vein drains into left renal vein. Right ovarian vein drains into inferior vena cava.
Reduced aortic-SMA angle where significant compression onto left renal vein between superior mesenteric artery (SMA) and aorta (nutcracker phenomenon) -mid part of left renal vein.

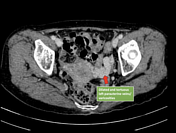
Corticomedullary phase as part of CT renal multi-phases (only limited to kidneys). The dilated left ovarian vein shows higher attenuation compared to adjacent inferior vena cava, which is another imaging sign to support the retrograde venous blood flow into the left ovarian vein toward pelvic veins as the collateral pathway to bypass the stenosis at the mid left renal vein.

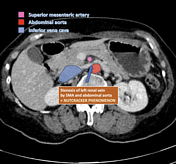

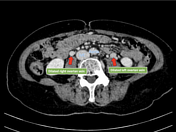

Annotated images showing the possible collateral venous pathways back towards the inferior vena cava via pelvic/uterine veins and the nutcracker phenomenon.
Case Discussion
Features consistent with pelvic congestion syndrome, which in this case is caused by compression of the left renal vein by SMA (known as the nutcracker phenomenon). As the patient presented with persistent microscopic hematuria as associated symptoms, this is referred to as nutcracker syndrome. This syndrome can lead to renal venous hypertension, resulting in the rupture of thin-walled veins into the collecting system with resultant hematuria.
The common clinical manifestations are left flank pain, hematuria, pelvic pain and gonadal varies.
Imaging findings of multiple dilated, tortuous para uterine veins with a width >4 mm or an ovarian vein diameter >8 mm are considered measurements to suggest this diagnosis.
In this case, the possible collateral pathway is via the left ovarian vein, down to the left para-uterine veins, right para-uterine veins, right ovarian vein then towards the inferior vena cava.
As the patient is symptomatic (hematuria), surgical treatment may be necessary to relieve the pain as well as to prevent renal vein thrombosis the known complication of nutcracker syndrome.
Identifying the pelvic congestion/shunting syndrome as part of the review area for female patients presented with hematuria (enlarged uterine veins in females) is crucial to look for the possibility of nutcracker phenomenon (which is a common finding even in asymptomatic patients). This can avoid further unnecessary investigation such as cystoscopy or ureteroscopy.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.