
Presentation
Severe abdominal pain for 2 weeks with detected sizable right-sided pelvic mass by ultrasonography.
Patient Data
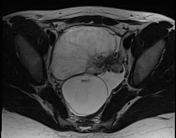







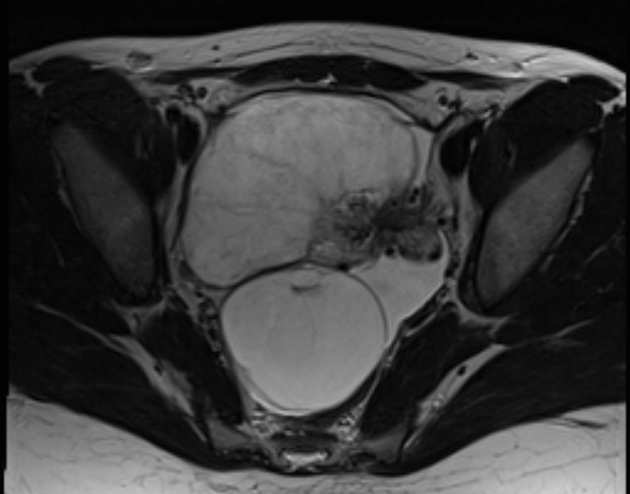
A sizable oval-shaped pelvic mass is seen attaining its blood supply from engorged left gonadal vessels reflecting enlarged left ovary reaching up to 250 cc (9.5 x 8 x 6.5 cm). It exhibits marked loss of the cortico-medullary differentiation sequel to marked edema and congestion, with residual peripherally located follicles. Diffuse reticular pattern of the intra-ovarian vascular tree reflecting blood stagnation reflecting massive ovarian edema. No diffusion restriction.
Whorly appearance of the related free edge broad ligament containing prominent fallopian tube which shows marked vascular congestion and tortuosity confirming twisted pedicle.
It’s seen prolapsing into the Douglas pouch at right paramedian position (sonographically suspected right adnexal lesion) pushing the uterus into an exaggerated AVF axis and effacing the right ovary posteriorly.
Mild free pelvic fluid is also noted.
The right ovary revealed a cystic lesion of 5.5 cm with clear content, thin wall, and no soft tissue component.
Case Discussion
Features that support the diagnosis of ovarian torsion are ovarian enlargement and edema, a twisted dilated tubular structure corresponding to the vascular pedicle (Whirlpool sign) and free pelvic fluid.
No associated adnexal solid or cystic lesions identified on imaging basis in order to be considered acting as a leading point. A long vascular pedicle could be the predisposing factor. It is a gynecological emergency and requires urgent surgical intervention to prevent ovarian necrosis.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.