
Presentation
Abdominal pain.
Patient Data


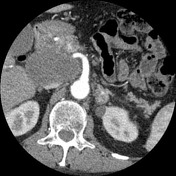
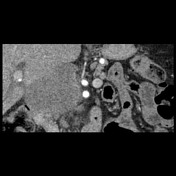
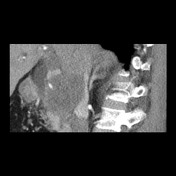
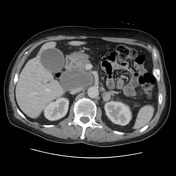

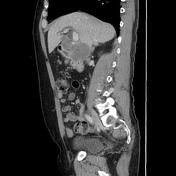
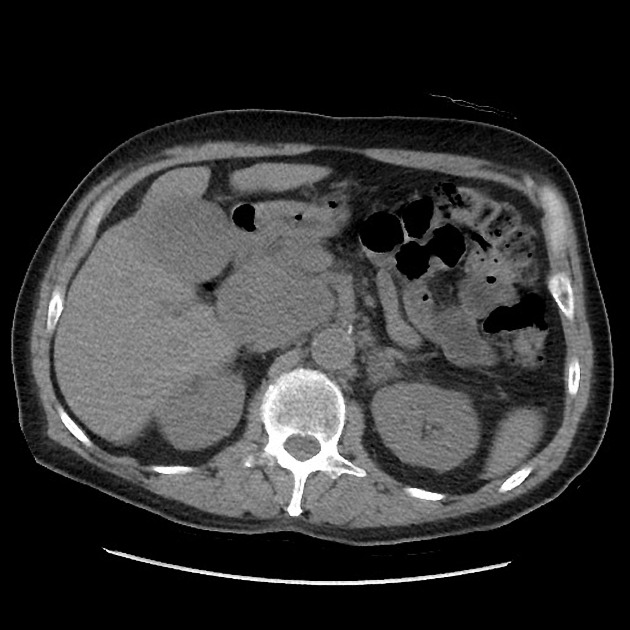
There is a large hypodense and hypovascular mass lesion arising from the pancreatic head/uncinate process measuring approximately 8.2 x 6.0 x 7.2 cm (longitudinal x AP x transverse). It completely encases but not obstructs the proximal portal vein and the right hepatic artery (which is replaced to the SMA - anatomical variant). It also involves in less than 180+ the left hepatic and left gastric arteries (also anatomical variant, with the left hepatic artery replaced to the left gastric artery) and abuts and compresses the left renal vein and IVC. There is compression against the distal CBD with mild upstream dilatation of the biliary tree (CBD measuring up to 10 mm in caliber). Multiple prominent retroperitoneal lymph nodes at this level measuring up to 1.5 cm in their short axis are noted.
The liver has otherwise unremarkable appearances, with no focal lesions. The left adrenal gland demonstrates a well-defined 2.3 cm nodule that has average attenuation of 12 HU; although it is nonspecific, this is more likely to represents a lipid poor adenoma. The right adrenal glands, spleen, and kidneys appear normal. The bowel has unremarkable appearances, no free fluid or free gas in the peritoneal cavity. No suspicious bone lesions. The imaged lung and pleural bases are clear.
Endoscopic ultrasound-guided FNA of periportal lymph node
Microscopy: The smears and cell block show a population of atypical columnar epithelial cells with enlarged, hyperchromatic nuclei, irregular nuclear membranes, prominent nucleoli and frequent mitotic figures arranged in cribriform formations within a background of necrotic debris. Immunohistochemistry, performed on cell block, demonstrates immunoreactivity of the cells with antibodies against CK 7. Immunohistochemistry with antibodies against CK 20, TTF-1, GATA-3, CDX-2, PSA and PSAP is negative.
Endoscopic ultrasound-guided FNA of periportal lymph node: Positive for malignancy. The features are those of metastatic adenocarcinoma. Tumor immunoprofile is in keeping with primary pancreatic origin.
Case Discussion
This case brings a bulky pancreatic head/uncinate process mass that extends into the hepatic hilum and is associated with large adjacent lymph nodes. There is no dilatation of the main pancreatic duct due to its location superior to the papilla. The bulky tumor is not completely clear if only arising from the pancreas or with a component of lymphadenopathy. Although atypical size and distribution, pancreatic adenocarcinoma was favored, with some considerations for lymphoma as a differential diagnosis.
Endoscopic ultrasound confirmed adenocarcinoma of the pancreas.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.