
Presentation
Persistent lump at base of left neck. Pain on swallowing.
Patient Data
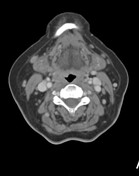



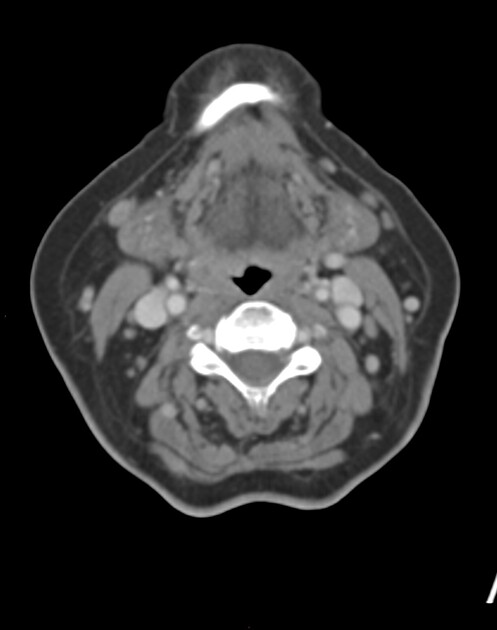
Large mass largely replacing the isthmus and left lobe of the thyroid. This measures approximately 40 x 50 x 50 mm. This is predominantly hypoattenuating to the normal thyroid, with some regions of probable necrosis. Coarse calcification along the medial margin may be intrinsic to this mass, or to other nodules in the thyroid. There is extrathyroid extension both anteriorly - involving the strap muscles in level 6 - and posteriorly - with invasion of the anterior tracheal margin.
Contact with the left internal jugular vein but no carotid space encasement.
Solid ipsilateral neck nodal disease in left levels 3 and 4, measuring 25 mm and 35 mm respectively.
Nodal disease also present in the upper mediastinum in both left and right upper paratracheal stations measuring around 15 mm. No nodal macrocalcification.
Despite the anterior tracheal invasion there is no airway narrowing with minimal early airway displacement. No definite oesophageal involvement.
No mass in the included aerodigestive tract. No other significant neck soft tissue abnormality. Normal included intracranial structures.
No pulmonary masses or concerning nodules. No pleural abnormality. No large / central PE. Mild coronary vessel calcification.
Normal included skeleton.
Case Discussion
Aggressive thyroid lesion, with probable necrosis and definite extrathyroid extension. Solid left neck lateral nodal disease with mediastinal nodal involvement. The age of the patient makes anaplastic malignancy a concern, although the clinical history may be longer standing.
Core biopsy of the left level 4 node demonstrated well differentiated papillary thyroid cancer, with no aggressive or poor prognostic features. Endoscopic examination confirmed anterior tracheal invasion, with no tumour seen in the proximal cervical oesophagus.
The patient was started on immunotherapy and is under surgical review.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.