
Presentation
Acute unilateral hip pain and immobility, no significant trauma.
Patient Data




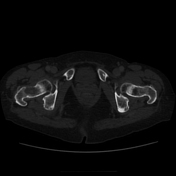
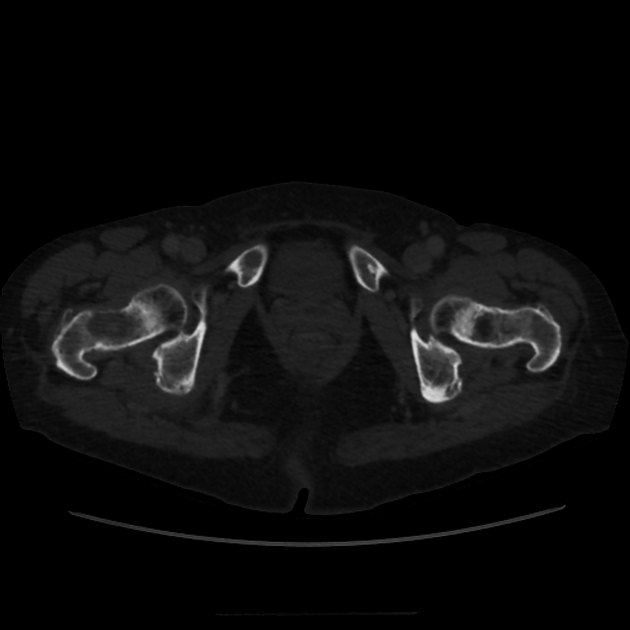
Basicervical right neck of femur fracture. Lucency at the fracture site is consistent with known metastasis here. Further metastases are seen involving the right acetabulum, left acetabulum and right inferior pubic ramus.
No distal femoral bone lesion.
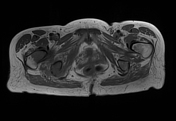

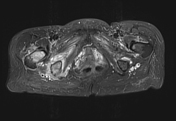
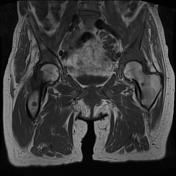
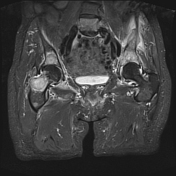
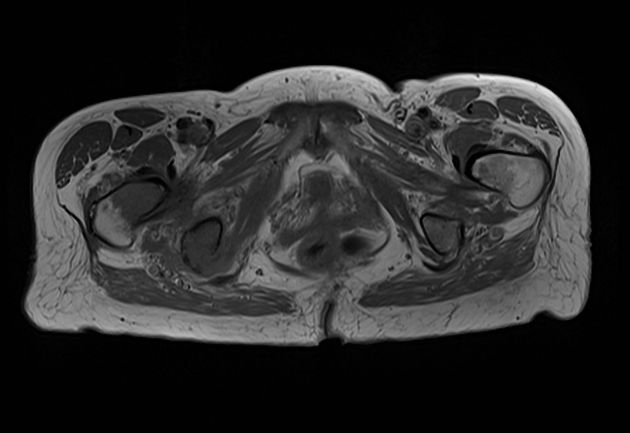
Widespread bone metastases involving the spine, pelvis and proximal femora

Necrotic appearing tumor around the right main and upper lobe bronchus extending into the mediastinum which is continuity with enlarged mediastinal nodes and extending into the subcarinal group.
Multiple bilateral scattered pulmonary nodules consistent with pulmonary metastases. Moderate right pleural effusion. Scarring at the left lung apex.
Multiple suspicious skeletal lucencies within the lumbar spine/sacrum in particular.
Case Discussion
Atraumatic hip pain in a patient with history of lung cancer diagnosed around 3 months previously.
Presentation XR Pelvis and Right Hip confirms pathological right neck of femur fracture and multiple focal lucencies within the bony pelvis.
MRI pelvis from 2 months prior shows widespread bony metastatic deposits, including full diameter involvement of the right femoral neck placing this area at particular risk.
CT from around 3 months prior to this acute presentation shows advanced right central bronchial carcinoma with evidence of mediastinal invasion, nodal disease and suspicious skeletal lucencies.
Patient underwent hemiarthroplasty and pathology from the right neck of femur sample confirmed adenocarcinoma, compatible with spread from the known lung primary.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.