
Presentation
Machete attack to the head.
Patient Data


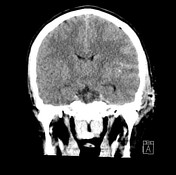
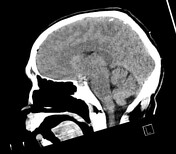
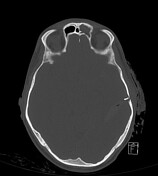
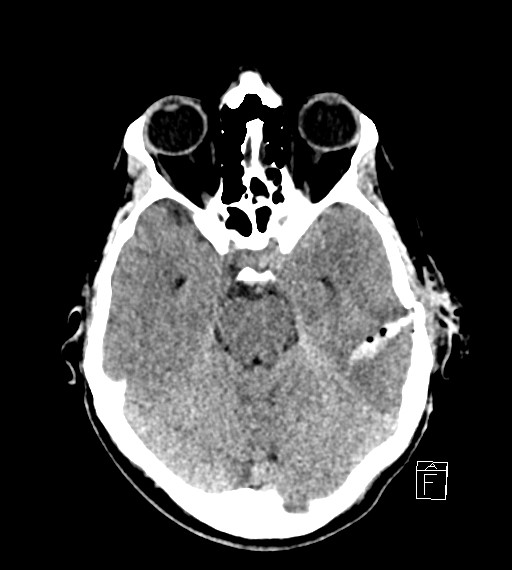
Non contrast CT head
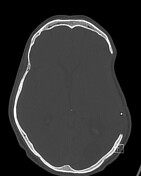
Long entry wound through the left temporal bone producing a complex, comminuted skull fracture, bone fragments extending into the brain parenchyma and associated pneumocephalus. The fracture involves the squamous and petrous portions of the temporal bone. A fracture through the condylar fossa of the temporal bone continues vertically and medially through the middle ear cavity and to the intracranial space. The carotid canal appears intact. Further comminuted fracture of the posterior left parietal and superior occipital bones. Associated overlying subcutaneous emphysema, soft tissue thickening and lacerations. Skin staples in the left scalp.
Large linear region of intraparenchymal blood in the parietal and temporal lobes, subarachnoid blood in the sylvian fissure and suprasellar cistern on the left and the suggestion of subdural blood over the left tentorium. There is no intraventricular blood evident.
Grey-white differentiation is preserved. There is no midline shift however there is decreased sulcation over the left cerebral convexity towards the vertex suggestive of early edema. Additionally there is fullness over the left medial temporal lobe and uncus concerning for early uncal herniation and similar appearance concerning for early left subfalcine herniation. The cerebellar tonsils sit above the foramen magnum The ventricles are symmetrical and slit-like. The basal cisterns remain patent.
The bony orbits appear intact. No intraorbital fat stranding, emphysema or soft tissue thickening. Hyperdense secretions within the left frontal sinus, mucosal thickening in the inferior maxillary sinuses.
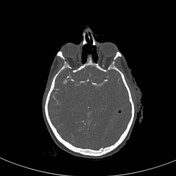
CT angiogram
There is a four-vessel aortic arch, the left vertebral artery arises directly from the arch. The extra cranial carotid and vertebral arteries demonstrate patency with no filling defect, aneurysmal dilatation or dissection.
The vertebral arteries form the basilar in typical fashion and the posterior circulation appears intact.
The internal carotid arteries also demonstrate a normal appearance of the terminal branches and the ACA and MCA appear intact. The circle of Willis is complete.
No evidence of active bleeding within the brain parenchyma.
Impression
Acute intraparenchymal temporoparietal lobe hemorrhage with left-sided subarachnoid hemorrhage as well as a possible trace subdural hemorrhage. No associated midline shift however there is evidence of decreased sulcation over the left cerebral convexity and probable early uncal and subfalcine herniation. Grey-white differentiation remains preserved.
Complex, comminuted left temporal bone fracture which involves the middle ear apparatus, comminuted posterior parietal and occipital bone fractures and the comminuted intra-articular mandibular fossa fracture.
The carotid canal appears intact and there is no evidence of active intracranial arterial bleeding.
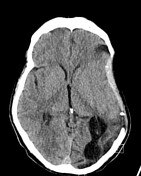


Comparison made with prior CT from 2 months prior.
The left frontal parietal craniotomy is redemonstrated. Surgical clips noted extending into the cerebral parenchyma in the left parietal region.
No evidence of acute intra or extra-axial hemorrhage. The left cerebral hemisphere volume loss with associated concave morphology to the cerebral convexity is stable. Gliotic changes involving the left parieto-occipital region.
The minimal midline shift to the right due to this is stable and measures 2 mm. The right frontal EVD tract is unchanged.
Case Discussion
The patient required a long ICU stay and multiple surgeries prior to ongoing rehabilitation.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.