
Presentation
A 3 week history of progressive shortness of breath, even on minimal exertion.
Patient Data

The heart is significantly enlarged (CTR = 0.64) with a globular contour. Appearances are concerning for a pericardial effusion.
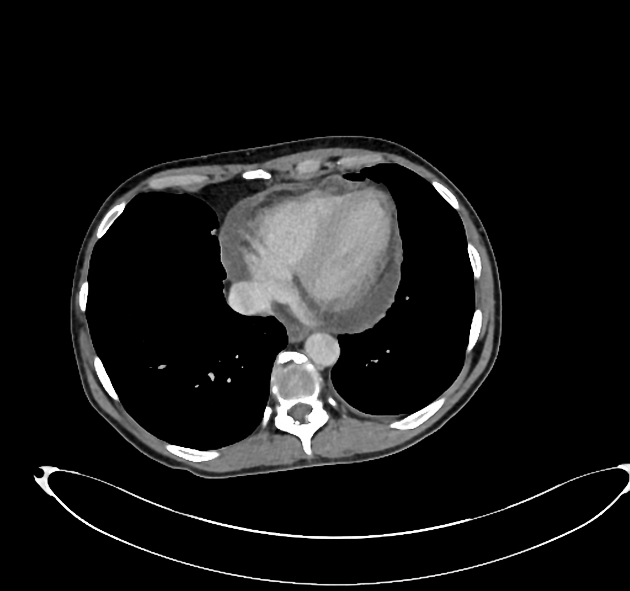
Axial slices through the chest, with contrast enhancement in the portal venous phase, showing a moderate volume pericardial effusion and an enlarged left paratracheal node.
Case Discussion
The patient was referred urgently for clinical review and an echocardiogram. The echocardiogram confirmed the pleural effusion.
Blood analysis revealed no evidence of acute coronary syndrome or heart failure. Similarly, there were no features of infection or uremia, and malignancy was excluded on computer tomography.
A pericardial drain was inserted, and 1750 mL of fluid accumulated. Samples of the fluid was sent for biochemical, microscopic, and immunohistochemical investigation, all of which were negative.
Repeat echocardiography confirmed trace pericardial effusion with no hemodynamic compromise.
The pericardial effusion was thought secondary to an underlying pericarditis.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.