
Presentation
A patient with acidosis and anaemia. Evaluate for intracranial haemorrhage.
Patient Data

There was no abnormal intraventricular or parenchymal hyperechogenicity. The caudothalamic groove is normal. There is a simplification of sulcation, and the gyral pattern is in keeping with the preterm state.

There is increased periventricular white matter echogenicity, more than the expected periventricular echogenic blush. Additionally, the choroid plexus bilaterally is somewhat heterogeneous, with heterogeneous fullness of the bilateral caudothalamic grooves. Although the ventricular system is not overly dilated, there has been an increase in calibre compared to the prior exam.
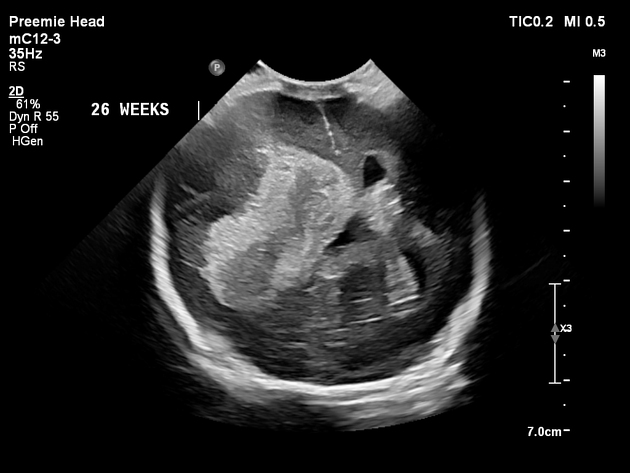
There is significantly increased hyperechogenicity likely within the right ventricle, however, now with more pronounced extension into the periventricular white matter. The periventricular white matter hyperechogenicity is now greater than the choroid plexus. Intraventricular haemorrhage extends into the third ventricle. The right lateral ventricle is effaced due to a leftward midline shift, and there is a large mass at the left lateral ventricle, worrisome for entrapment.

There is haemorrhage in the right lateral ventricle with involvement of the right periventricular white matter. There is a persistent leftward midline shift and a persistent extension of haemorrhage into the third ventricle. The asymmetric increased calibre of the left lateral ventricle has not significantly changed compared to prior. The left choroid plexus is again somewhat heterogeneous, and cord plexus haemorrhage is not excluded.

There has been interval enlargement of the ventricles, including the third and fourth ventricles.
There is a residual evolving haemorrhage in the right ventricle, with probable trace residual haemorrhage in the left ventricle. The midline structures are distorted due to the hydrocephalus and a slight leftward midline shift.
There is right periventricular encephalomalacia, which appears to be contiguous with
the right lateral ventricle.
Case Discussion
This is a case demonstrating progressive findings of a large intracranial haemorrhage to severe periventricular leukomalacia in a preterm infant. Given the provided history, the haemorrhage may be secondary to a germinal matrix haemorrhage grade 4 or haemorrhagic conversion of ischaemic tissue, though the former is considered more likely given the early enlargement and heterogeneity of the choroid plexus.
Co-author:
Joshua Goldwag


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.