
Presentation
Headache and vomiting.
Patient Data


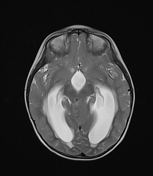
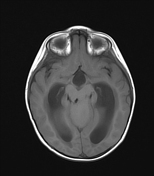
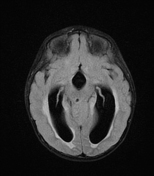
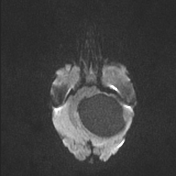
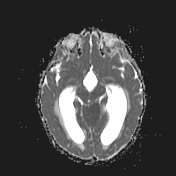
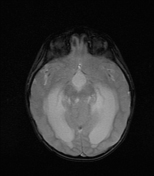
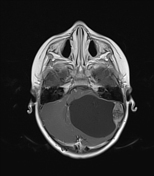
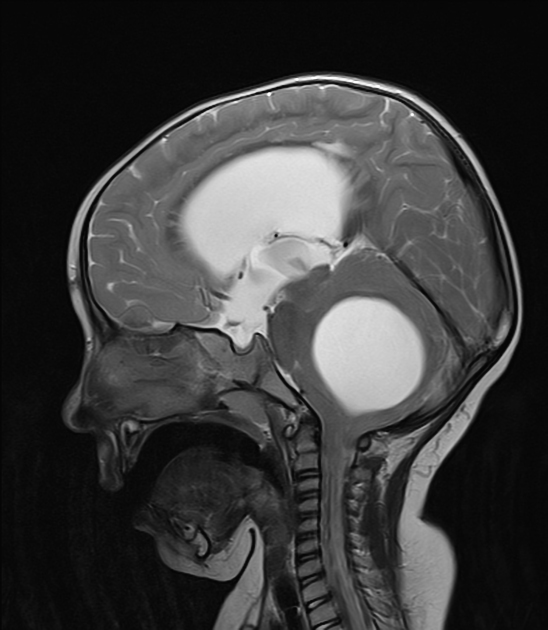
There is a large, well-defined, predominantly cystic mass with a solid mural nodule in the left cerebellar hemisphere. The solid mural nodule of the mass lesion shows enhancement in post-contrast images. No diffusion restriction. No significant peri lesional edema.
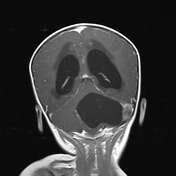
The lesion causes a mass effect on the 4th ventricle with resultant proximal tri-ventricular acute hydrocephalus evident by transepyndymal CSF leakage. Other features of increased intracranial pressures are also present like partial empty sella sign, Prominent CSF spaces around the optic nerves, and optic disc bulging.
Case Discussion
Considering the patient's age and imaging features, The most likely diagnosis is a pilocytic astrocytoma; a low-grade tumor of the posterior fossa in the children. The clinical features of headache and vomiting are related to the increased intracranial pressure. The patient underwent surgery and after 4-year follow-up; she is currently well without any deficit. No pathology report is available.
The imaging differential diagnosis can be hemangioblastoma, again a cystic mass with a solid mural nodule, but it occurs in middle age and is often associated with Von Hipple Lindau disease.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.