
Presentation
Not available.
Patient Data
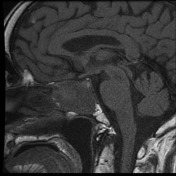

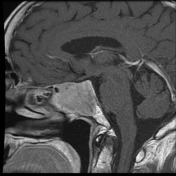
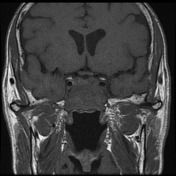

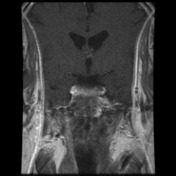

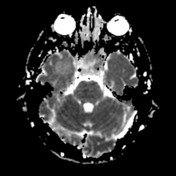
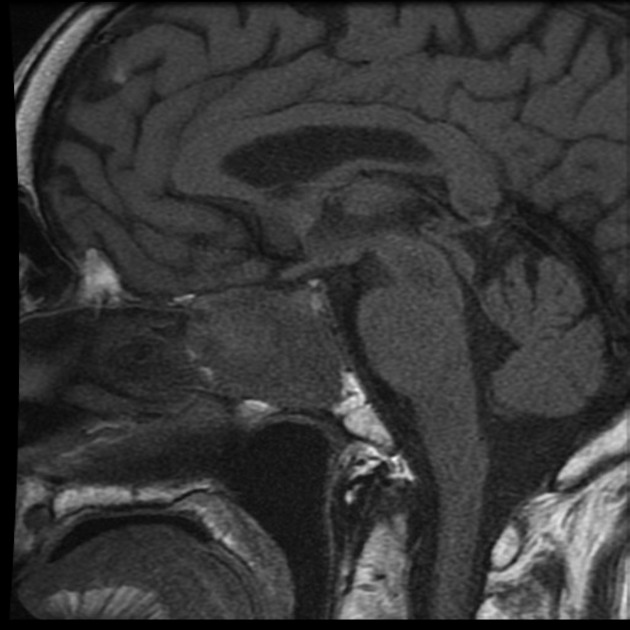
A tumour fills an expanded sella, and most of the sphenoid sinus, and extends into the clivus, of heterogeneous appearance with different regions having different signal characteristics. Seen posteriorly and superiorly, is tissue consistent with residual normal pituitary, of different signal intensity on unenhanced T1- weighted scans, with contrast enhancement, particularly on the dynamic scans typical of pituitary. The bulk of the tumour is of lower signal intensity on T1, enhances uniformly, bulges into the LEFT cavernous sinus, although does not encase the internal carotid artery. Both internal carotid arteries have normal flow voids and are not significantly stenosed on spin-echo sequences. There is suprasellar extension, but there is no compression of the optic chiasm and no significant contact/compression of the optic nerves.
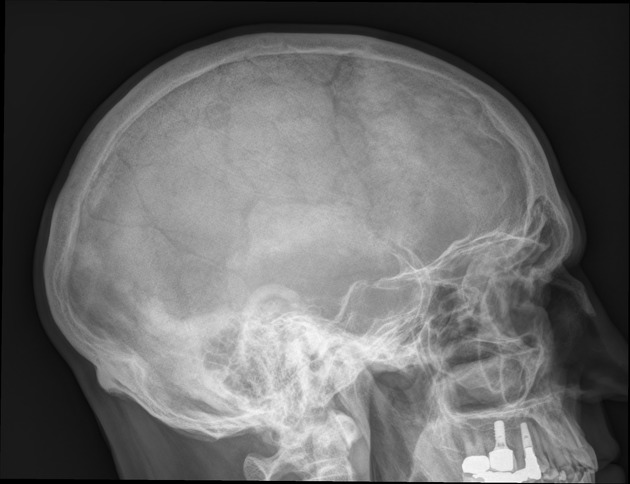
The pituitary fossa is expanded with erosion of the anterior and posterior walls as well as the floor of the fossa.
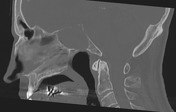

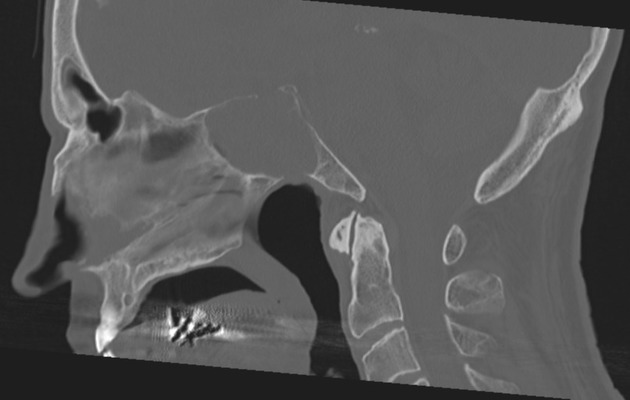
Expansile pituitary mass measuring up to 3.5 cm in diameter is identified. This causes marked bony expansion of the pituitary fossa with erosion of the floor. The ventricular system is of normal size and is midline in location.
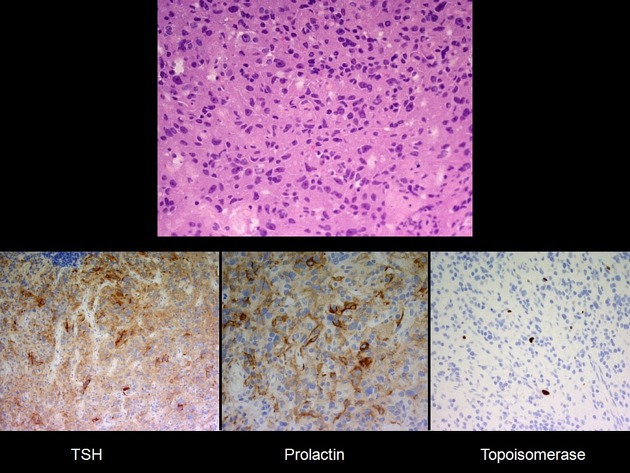
MICROSCOPIC DESCRIPTION: All the sections show a moderately cellular pituitary adenoma comprising sheets and nests, surrounded by vascularised stroma. The tumour cells have enlarged pleomorphic nuclei, prominent nucleoli and small amounts of eosinophilic cytoplasm. No normal anterior pituitary gland tissue is present. The tumour cells show patchy positivity with TSH and prolactin. The Ki-67 index is about 1%. Immunostains for GH, ACTH, LH and FSH are negative. The features are most consistent with silent subtype 3 adenoma. The slides have been reviewed by A/Prof. Gonzales.
DIAGNOSIS: Pituitary: Features most consistent with silent subtype 3 adenoma.
Case Discussion
Despite the presence of residual pituitary gland, the most probable diagnosis on imaging is of a pituitary macroadenoma with predominant inferior growth, which was later confirmed on histology. While there are differential imaging diagnoses, such has solid craniopharyngioma, osseous lesions of the sphenoid, and even central skull base meningioma, these are all considered much less likely.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.