
Presentation
One month blurred vision and increasing headache.
Patient Data


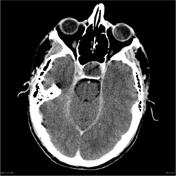

Large predominantly low density pituitary fossa mass is noted which extends into the suprasellar cistern. The lesion is predominately low density, however, does demonstrate a peripheral high attenuation rim with some heterogenous signal intensity is seen particularly in the anteroinferior margin with possibly a small nodule adjacent to this. No calcification is identified. The pituitary gland itself cannot be identified. The sella is grossly expanded, however, no definite bony destruction is identified.


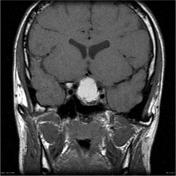


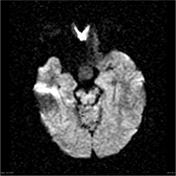

A 19 x 23 x 25mm ovoid mass lesion is seen in the pituitary fossa with suprasellar extension. The mass is not clearly separate from the anterior portion of the pituitary, which cannot be identified. A solid component is located anterolaterally (towards the left) and this component enhances. The optic chiasm is markedly compressed, draped over the superior aspect of the mass lesion. The mass is T1 and T2 hyperintense centrally with no significant enhancement post contrast. There are a few fine internal septations. No restricted diffusion within the mass. No calcifications.
The remaining imaged brain, including posterior fossa structures, are normal.
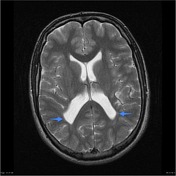
The white matter in the peri trigonal regions is thinned with undulation of the lateral margins of the lateral ventricles.
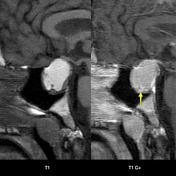
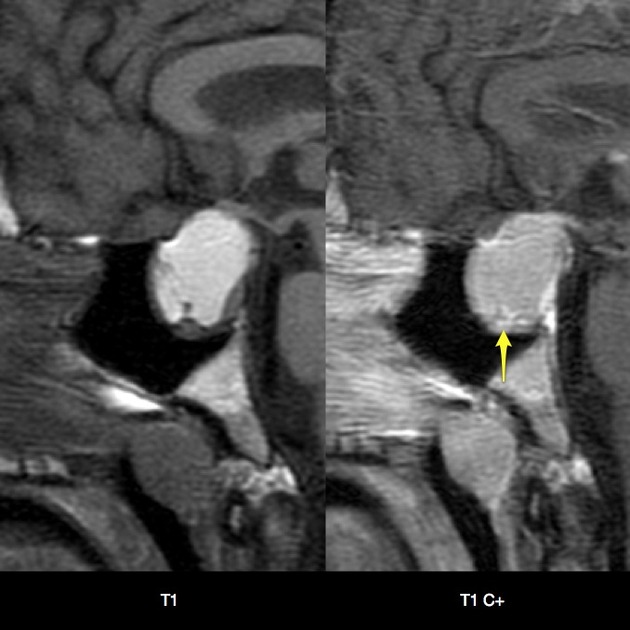
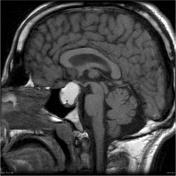
Pre and post contrast T1 sagittal images demonstrate peripherally enhancing nodules (yellow arrow).
Blue arrows demonstrate thinned white matter with regions of T2 hyperintensity (blue arrows). The ventricular margins in these regions are undulated, features fairly characteristic of the sequelae of perinatal periventricular leukomalacia.
This patient went on to have transphenoidal surgery.
Histology
Paraffin sections show fragments of a moderately hypercellular adenoma. Tumor cells have regular nuclear features and a variable amount of pale cytoplasm and are arranged in trabeculae and diffuse sheets intersected by thin-walled capillaries. No mitotic figures or areas of necrosis are seen. No normal anterior pituitary tissue is included. Immunohistochemistry shows moderately strong cytoplasmic staining for FSH in tunmour cells. No staining for growth hormone, prolactin, ACTH, LH, TSH or CAM5.2 is seen in tumor cells. The features are of a non-functioning gonadotroph cell adenoma. The topoisomerase labeling index is <1%.
FINAL DIAGNOSIS: Pituitary tumor: Non-functioning gonadotroph cell adenoma.
Case Discussion
This case demonstrates the typical appearances of a necrotic pituitary macroadenoma, which can be challenging to differentiate from a craniopharyngioma or pituitary hemorrhage.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.