
Presentation
Presents with acute abdominal pain. US shows marked right hydronephrosis and hydroureter. CT for clarification of the cause.
Patient Data

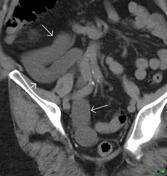

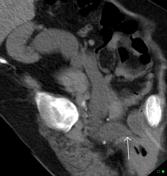

Markedly distended right renal pelvis and ureter (up to 4 cm in diameter) with tortuosity down to a tapered distal ureter (arrow) at the bladder. No calculus and minimal calyceal dilatation without cortical atrophy as would be expected in a chronically obstructed or refluxing collecting system.
Case Discussion
Megaureter in an adult is often due to distal obstruction, occasionally gross reflux or commonly idiopathic (i.e. developmental). Even if idiopathic the patient can be symptomatic due to urinary stasis leading to recurrent infection or calculi. The key to diagnosing an idiopathic cause is the absence of obstruction on a frusemide nuclear renal scan, lack of reflux on MCUG and the absence of calyceal dilatation and renal parenchymal thinning as would be expected in a chronically obstructed kidney that could lead to such ureteric dilatation.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.