
Presentation
Evaluate stent position, right renal mass.
Patient Data




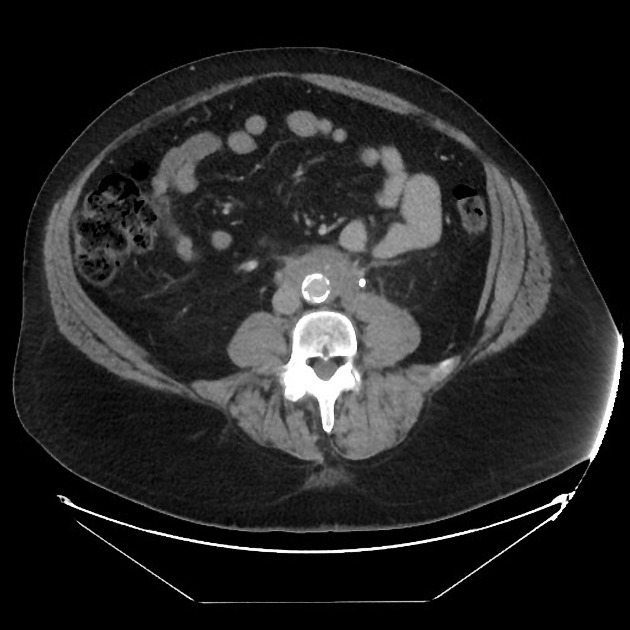
Periaortic soft tissue infiltration extending from slightly below the aortic bifurcation to slightly above the IMA. Medialization of the ureters with stenting of the left ureter, mild to moderate hydronephrosis, and delayed nephrogram. No adenopathy. Aorta is not “lifted” by the soft tissue.


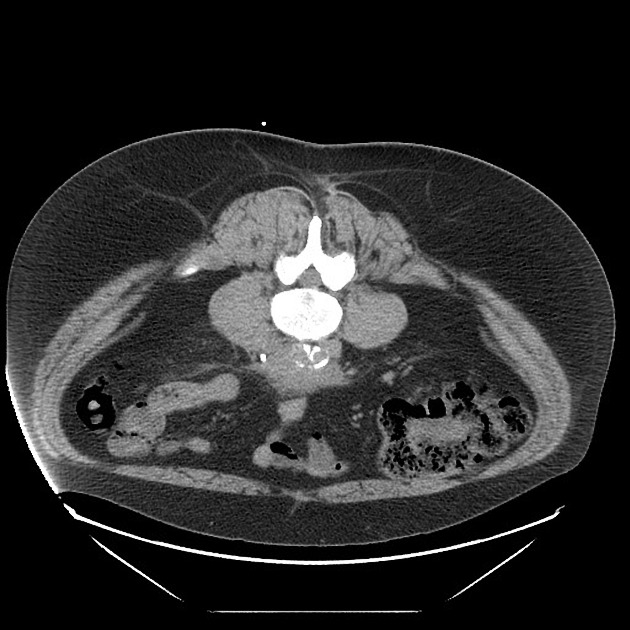
Left posterior paraspinal approach for biopsy. Notice the relationship of the needle, left ureteral stent, and aorta.
Case Discussion
Typical case of retroperitoneal fibrosis. This was confirmed with CT-guided biopsy which demonstrated “fibroadipose tissue with fibroblasic/myofibroblasic proliferation, fibrosis and mixed chronic inflammation including plasma cells consistent with RPF; not sufficient for igG4-related.”
RPF usually starts around L4-L5 at the bifurcation and ascends, medializing and obstructing the ureters. While retroperitoneal lymphoma is a consideration, it typical “lifts” the aorta and displaces the ureters, NOT medializes them toward the mass.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.