
Presentation
The patient has known RPF. For follow-up post utereolysis for ureteric obstruction.
Patient Data
Age: 60 years
Gender: Female


Download
Info
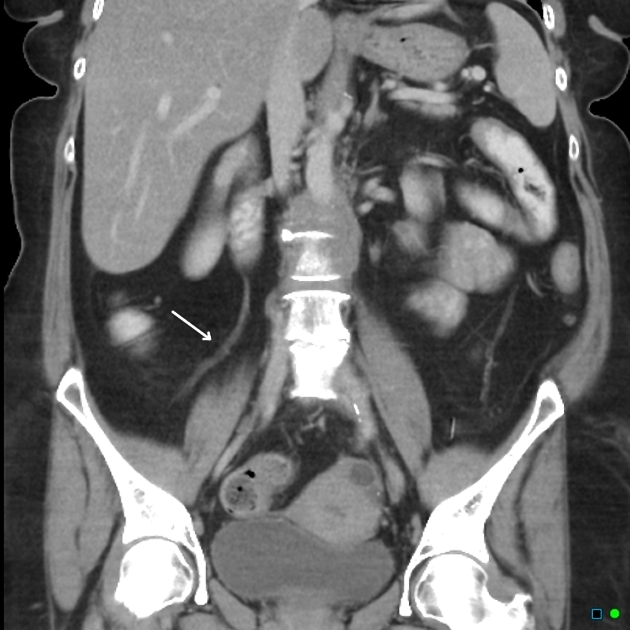
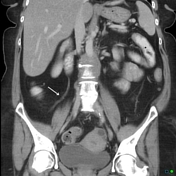
Cuff of enhancing tissue surrounding the abdominal aorta indicative of fibrosis. No aneurysmal dilatation of the aorta. Both ureters are laterally displaced especially on the right post ureterolysis (note the surgical clips). Neither kidney is hydronephrotic.
Case Discussion
Ureteric obstruction is a major complication of RPF and may require ureterolysis. The surgeon will strip the ureters away from the fibrosis and place them out laterally to avoid further extrinsic compression (in some cases wrapping them in omentum).


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.