
Presentation
Lumbar back pain and perianal numbness.
Patient Data



The examination was aborted prior to contrast enhanced scans due to patients inability to lie flat.
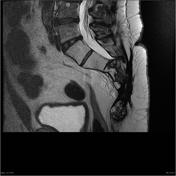
Transitional anatomy, with rudimentary disc at S1/S2. The cord terminates normally at L1/2.
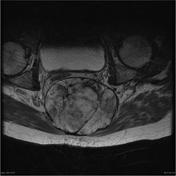
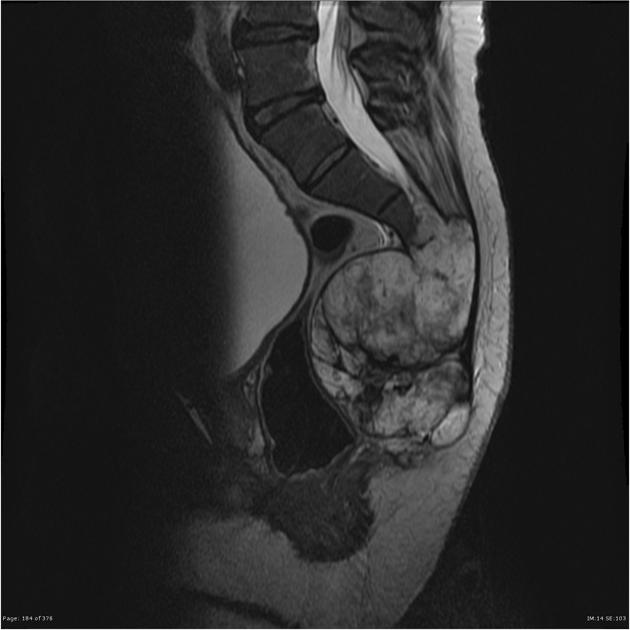
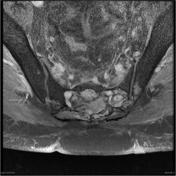
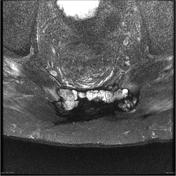
A large circumscribed midline mass destroys the sacrum from the level of the inferior aspect of S3, with cranial extension to entirely occupy the sacral canal to the level of S2/3. The S1 and S2 nerve roots are intact, but S3 to S5 are not distinguishable. The mass has dimensions of 7.7 x 10 x 12.7 cm (AP x transverse x craniocaudal) and bulges anteriorly to displace the rectum, but is well circumscribed with preservation of the intervening fat plane.
The mass is of heterogeneous very high T2 and intermediate to high T1 signal suggesting proteinaceous or blood products. and contains internal septae which split the tumor into incomplete lobules. No enlarged pelvic lymph nodes identified.
Vertebral body height and alignment are normal. Normal marrow signal.
There are mild endplate degenerative changes and small concentric disc bulges at L3/4, L4.5 and L5/S1, however the canal, subarticular recesses and neural foramina are adequate.
Conclusion:
Large circumscribed midline mass arising from the distal sacrum with obliteration of the S3 to S5 nerve roots. Unfortunately the mass is incompletely characterized as contrast enhanced sequences could not be performed. This mass is compatible with chordoma, and biopsy is recommended.


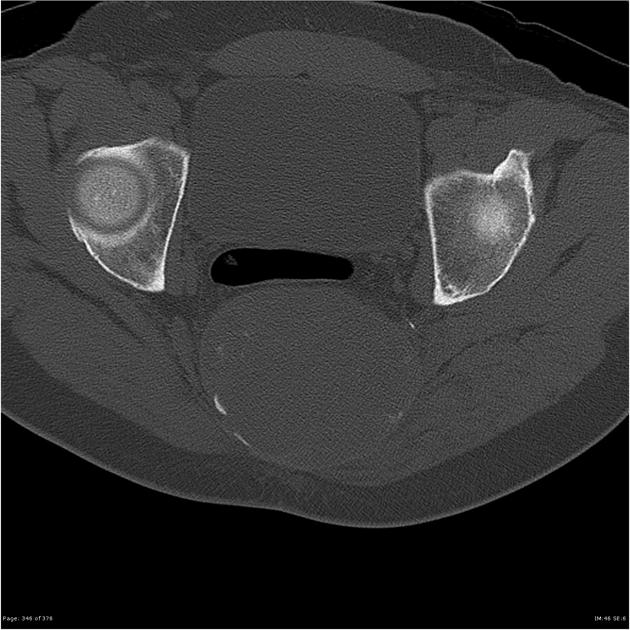
A large midline mass with dimensions of 10.1 x 8.2 x 11 .7 cm (transverse x AP x longitudinal) destroys the distal sacrum from the level of the inferior aspect of S3, and extends cranially to fill the sacral canal to the level of S2/3. The mass is well circumscribed and internally heterogeneous, but predominantly of fluid density with internal septations and coarse calcification. The rectum is flattened and displaced anteriorly but the intervening fat plane is preserved.
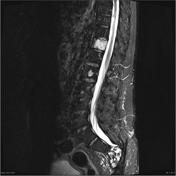








Comparison is made with the previous imaging done in November 08 and there has been debulking of the tumor. On the current imaging no tumor is seen anterior to the level of the sacrum. There is still extensive fairly well demarcated irregular whirled mixed signal tumor seen extending from the level of S2 to the coccyx. This also extends laterally to just below the level of the ischial spine in the ischiorectal fossae. There is no involvement of the rectum. The pararectal tissues demonstrate mild enhancement, which is probably postsurgical and post radiotherapy.
The lower lumbar spine and proximal sacrum are normal with normal exiting nerve roots and thecal sac.\
Multiple high T2 signal deposits are seen in the vertebral bodies the largest of which is at the level to T5 in a paravertebral location.
CONCLUSION:
Debulking has occurred surgically with no tumor now seen anterior to the anterior spinal line. The lateral/width extent is similar to that seen pre- surgically. The tumor is about 1/5th of its previous size. Most of the tumor is within the ischiorectal fossae bilaterally and within the S2 to S5 sacral elements. No rectal involvement.
The patient went on to have incomplete resection of the mass.
Histology
MACROSCOPIC DESCRIPTION:
"Sacral tumor": Multiple pieces of rubbery pink and fawn tissue up to 150mm in gteratest dimension. Areas of gelatiknous material are noted as well as gritty foci consistent with bone. Areas of hemorrhage are also seen.
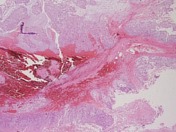
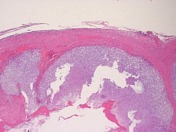
MICROSCOPIC DESCRIPTION:
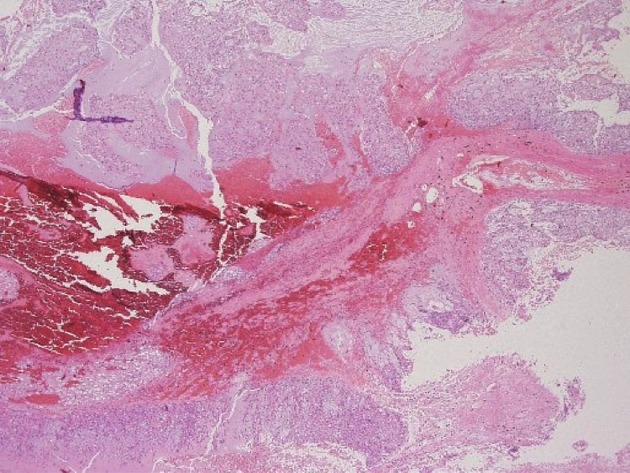
The sections show a densely hypercellular tumor. This is composed of cells with small round and oval vesicular nuclei. The immediately perinuclear cytoplasm is densely eosiniphilic but vacuolated peripherally. This vacuolation imparts a physalliferous appearance. Tumor cells are arranged in small solid aggregates and cords within mucinous material. Lobules of tumor are separated by coarse collagenous septa and have a pushing margin with adjacent soft tissues. Invasion of bone is noted in some fragments. Scattered mitotic figures are identified. No tumor necrosis is seen. Areas of recent hemorrhage are noted in some tumor lobules. No mature cartilage is identified. The overall features are of chordoma.
FINAL DIAGNOSIS: Chordoma.
The patient remained well, until 5 years after initial presentation he noticed a lump growing under the left scalp.


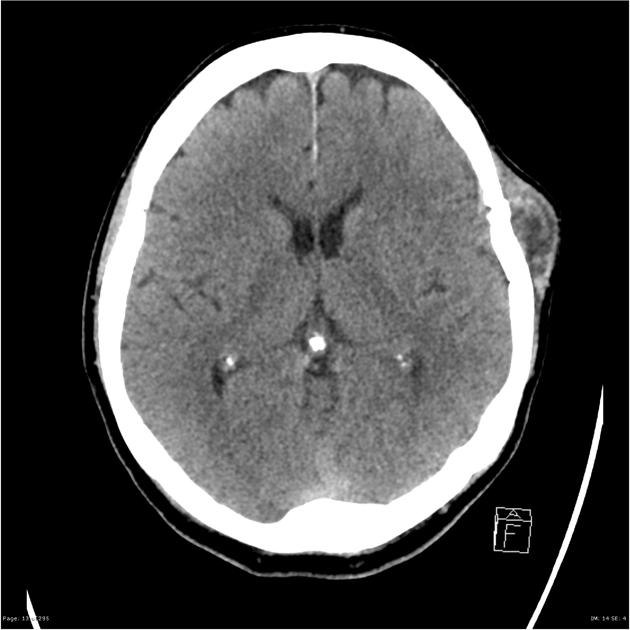
Multiple skull vault masses are present, the left parietal one being largest and most easily seen.
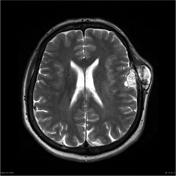
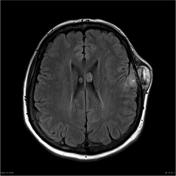
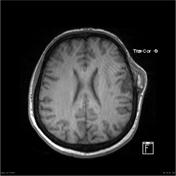

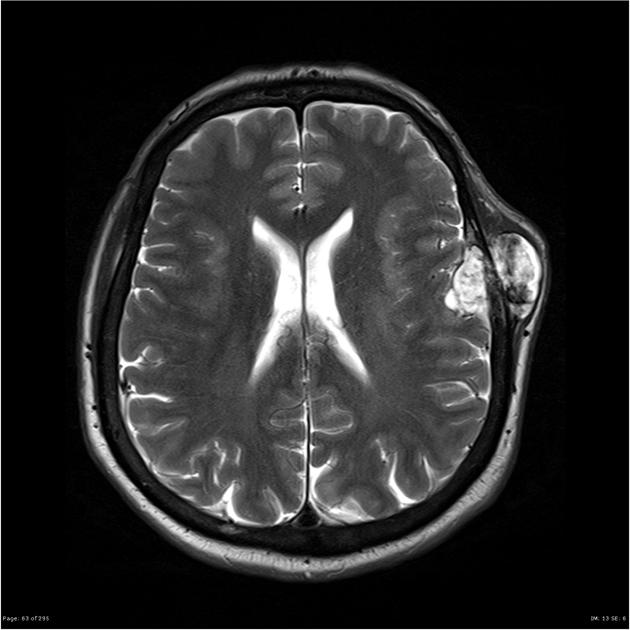
Multiple expansile enhancing calvarial lesions are identified, in many areas breaching inner table. The largest lesion is in the left frontal parietal region with an total dimensions of 4.6 x 5.2 cm with a 4.6 x 2.1 cm durally based component indenting the left posterior frontal lobe. Another large lesion at the posterior right vertex measures 3.8 x 4.4 cm in axial dimension with either invasion or marked compression of the superior sagittal sinus. These masses are of high T2 signal and demonstrate heterogenous contrast enhancement.
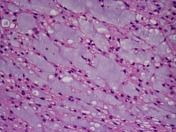
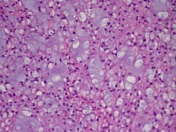
MACROSCOPIC DESCRIPTION: Six hemorrhagic gelatinous fragments.
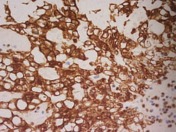
MICROSCOPIC DESCRIPTION: The sections show an epithelioid tumor, forming cords, embedded in prominently myxomatous stroma. The tumor invades into the dura and there is full thickness involvement of the skull bone. The tumor cells have mildly enlarged and hyperchromatic ovoid nuclei, small nucleoli and small amounts of eosinophilic cytoplasm. Scattered physaliferous cells are seen and they show cytoplasmic vacuolation. Lymphovascular invasion is absent. The tumor cells are CAM5.2 and S-100 positive, in keeping with chordoma. The tumor appears to be clear of the outer dural and bony margins. The tumor on the outer part of the skull bone is covered by a layer of fibrous tissue and skeletal muscle. It has not infiltrated through this outer margin.
DIAGNOSIS: Metastatic chordoma, completely excised with clear dural and bony margins.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.