
Presentation
Left flank neuropathic pain at T10 level.
Patient Data



Note made of transitional anatomy. There are 7 cervical vertebrae,
13 thoracic type
vertebrae with 13 pairs of ribs, and 5 lumbar type vertebrae.
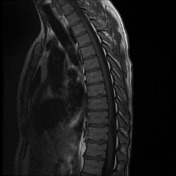
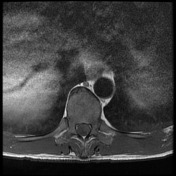
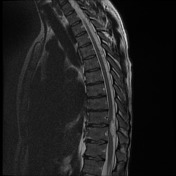
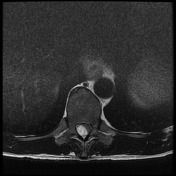
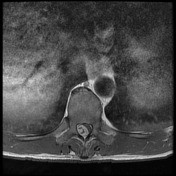
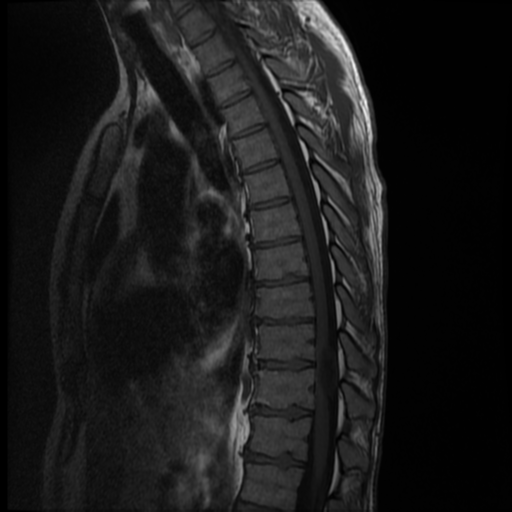
At T10/11 there is an ovoid intradural extramedullary mass which causes leftward displacement and severe compression of the cord, with subtle T2 hyperintensity in the adjacent cord. The mass is vividly T2 hyperintense and T1 hypointense, with vivid enhancement but irregular central region of non-enhancement. There is no extension into the right T10/11 foramen. No dural tail of enhancement.
No further mass or region of pathological enhancement. The remainder of the cord demonstrates normal signal, and there is no thoracic disc herniation.
T2 sagittal screening images through the lumbar spine have been performed, which demonstrate 8 mm L4/5 retrolisthesis of L5/S1 anterolisthesis in the context of bilateral L5 pars defects and bilateral L4/5 facet arthropathy. This does not cause canal stenosis or neural impingement.
Conclusion
Right posterolateral intradural extramedullary mass at T10/11 level causes severe cord compression and edema. Lesion is likely neurogenic tumor; signal characteristics would be very atypical for meningioma.
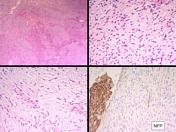

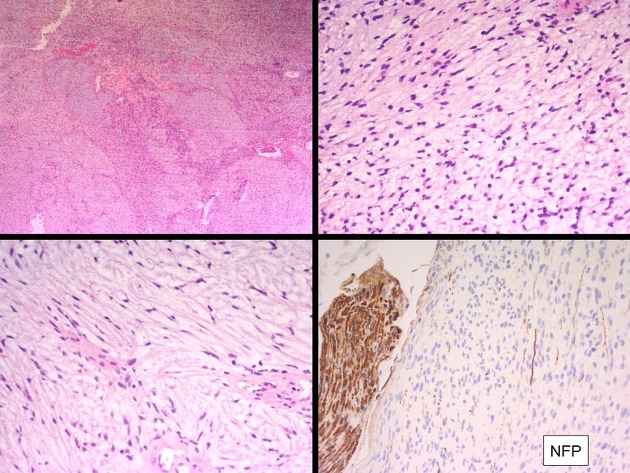
MICROSCOPIC DESCRIPTION: Paraffin sections show a moderately hypercellular neurofibroma. Tumor cells have mildly pleomorphic vermiform nuclei with delicate and coarse bipolar processes. These are dispersed haphazardly within a myxoid stroma. No mitotic figures, densely hypercellular areas or areas of necrosis are identified. Tumor is enclosed within a thin fibrous capsule. No extracapsular extension of tumor is seen.
DIAGNOSIS: T10-11 ?neurofibroma: Neurofibroma.
Case Discussion
This case illustrates a spinal neurofibroma, which is a benign, localized, and peripheral nerve sheath tumor.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.