
Presentation
Presented with headache and bitemporal haemianopia.
Patient Data
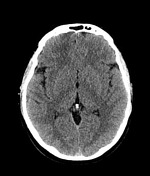

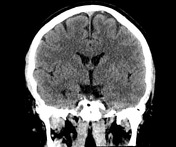


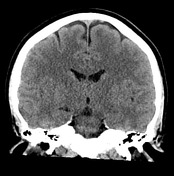
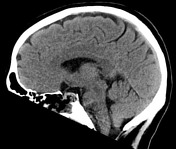
Well-circumscribed, slightly hyperdense pituitary fossa tumor with expansion of the fossa and suprasellar extension.
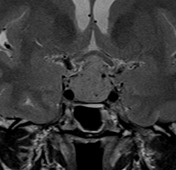

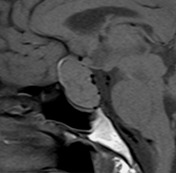
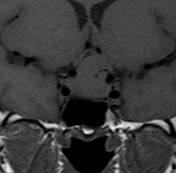
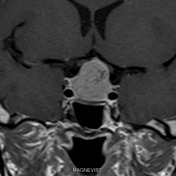
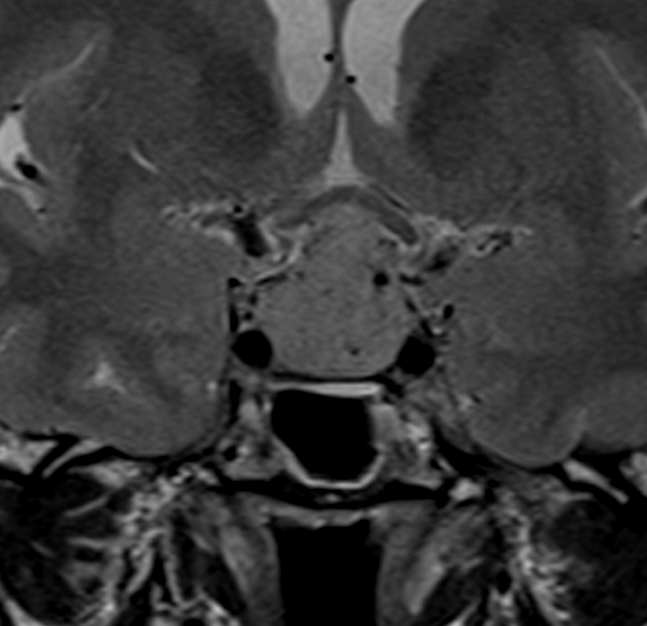
Mildly T2 hyperintense pituitary fossa tumor with predominantly solid, homogeneous enhancement, expanding the fossa and with suprasellar extension. Mild flattening of the optic chiasm and optic nerves. No evidence of cavernous sinus invasion.


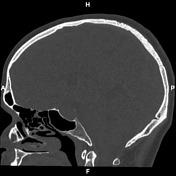
Post transsphenoidal resection of pituitary fossa tumor. Small volume blood products in the pituitary fossa. No evidence of post operative complication.
Microscopic description:
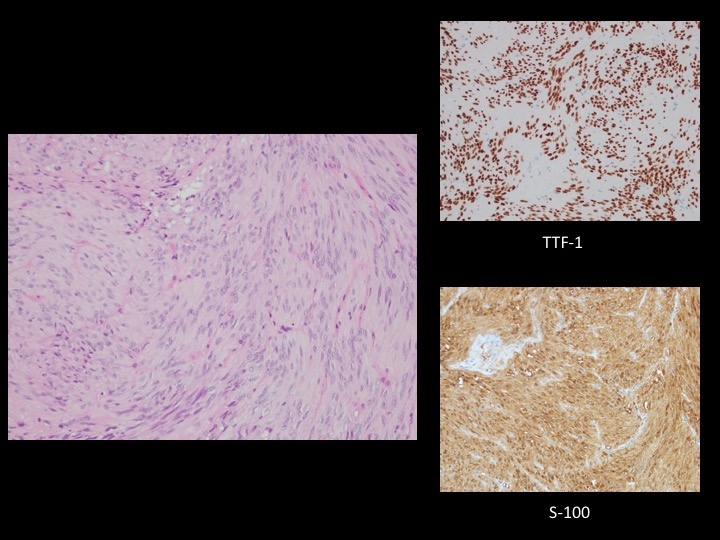
Paraffin sections show fragments of a moderately hypercellular tumor. This is composed of plump spindle cells arranged in loose fasciculi in a fibrous and vascular stroma. A palisaded arrangement of nuclei is noted in some areas. No mitotic figures or areas of necrosis are seen. No normal anterior pituitary tissue is included.
Immunohistochemistry shows strong nuclear staining for TTF-1 in tumor cells and strong cytoplasmic staining for S-100 protein. No staining for GFAP, synaptophysin, SOX10 or epithelial membrane antigen (EMA) is seen in tumor cells. The topoisomerase labellingindex is <1%. The features are of spindle cell oncocytoma.
Diagnosis: spindle cell oncocytoma.
Case Discussion
Spindle cell oncocytoma is a rare primary tumor of the pituitary gland, not distinguishable from adenoma on imaging.
Interwoven fascicles of elongated spindled cells are typical of histology.
Lacks staining for cytokeratins, pituitary hormones, or neuroendocrine markers.
Usually stains for S100 and thyroid transcription factor 1 (TTF1).
The histogenesis of the tumor is not completely understood; it is not clear if the cell of origin is in the anterior or posterior pituitary.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.