
Presentation
Young patient presented to vascular surgery clinic complaining of numbness in fingers and pins and needles which occurs lying with arms overhead in bed or after prolonged overhead sport or work activity. Bilateral symptoms had delayed consideration of thoracic outlet condition. Neurological examinations and cervical MR normal.
Patient Data


Technique
Contrast enhanced MR angiography in arms up and down positions using 2 separate Gadolinium contrast bolus injections.
Arms Down
Normal contrast flow through the subclavian arteries.
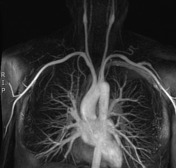
Arms Up
Focal occlusion to contrast flow at the level of both scalenus muscles, more severe on the right. The patient is right-handed and has more pronounced right-sided symptoms.
Case Discussion
Arterial thoracic outlet syndrome is a rare condition with congenital and acquired causes:
-
congenital causes:
- cervical rib
- aberrant scalenus anterior or intermedius muscles or fibrous bands relating to the muscles
- bony compression from abnormal transverse process, clavicle or osteochondroma
-
acquired causes:
- tumor / metastatic deposit
- trauma
- infection (compression from an abscess)
Radiological investigation:
- cervical spine radiographs
- supplementary thoracic outlet view to clarify the presence of cervical ribs
- MR or CT angiography in the arms up and down positions
Frequently these investigations follow more common MR C-Spine for presumed radicular cause of the patient's symptoms. In some cases, the findings can be confounding due to the high prevalence of disc osteophyte disease in the background population.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.