
The term bone tumour can be applied to a bewildering number of entities including primary and metastatic neoplasms as well as a variety of metabolic, developmental, lymphoid, reactive and tumour-like lesions that affect bone1-4. Hence, there are a wide variety of radiological appearances.
A systematic approach taking into account location, patient demographic and imaging appearances can often substantially narrow the differential. This is especially important if the mass is a benign "don't touch" lesion that could be safely ignored or observed.
This is an overview article; for more information please refer to the articles on each subtype described below.
On this page:
Epidemiology
Different tumour types have different epidemiological manifestations. Primary bone tumours are rare and are vastly outnumbered by metastases and haematopoietic tumours. The true incidence of primary bone tumours is difficult to determine due to their rarity and because most benign bone tumours are asymptomatic and go undetected 2,8,9.
Of the primary malignant bone cancers, the most common are osteosarcoma (35%), chondrosarcoma (30%), and Ewing sarcoma (16%) 5. These have different age distributions but there is a slight male predominance with a ratio of 1.3:1.
Clinical presentation
Benign bone tumours are often asymptomatic and identified incidentally. Others, however, can produce pain, cause a slow-growing mass, or result in a pathologic fracture 8.
Pathology
Most primary bone lesions are benign solitary phenomena, with a propensity for the long bones of the extremities 8. The presence of multiple bone lesions should raise suspicion for other entities, with metastases and multiple myeloma being the most common osteolytic lesions in patients older than 30 years 1,3.
There are numerous individual tumour entities which come under the umbrella term "bone tumour". For a formal and updated classification of bone tumours, see WHO classification of tumours of bone. They can broadly be divided into:
-
bone-forming tumours
-
cartilage-forming tumours
-
fibrous bone lesions
-
bone marrow tumours
-
other bone tumours or tumour-like lesions
-
miscellaneous
-
radiation changes
radiation-induced bone growth
Radiographic features
The radiographic appearance of the lesion provides essential information in differentiating bone tumours, with patient age being the most important clinical clue. The most reliable indicator in determining whether a lesion is aggressive (typically malignant) or nonaggressive (typically benign) is the zone of transition between the lesion and the adjacent normal bone 3.
Please see the describing a bone lesion and aggressive versus non-aggressive bone lesion articles for more detail.
Plain radiograph
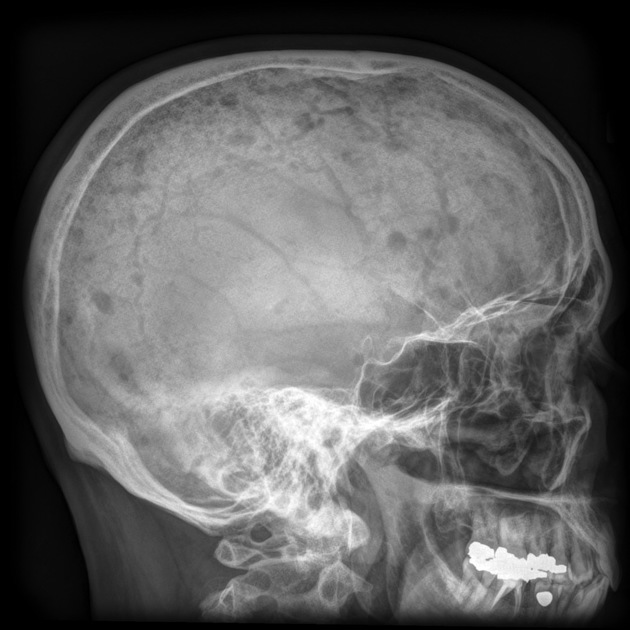
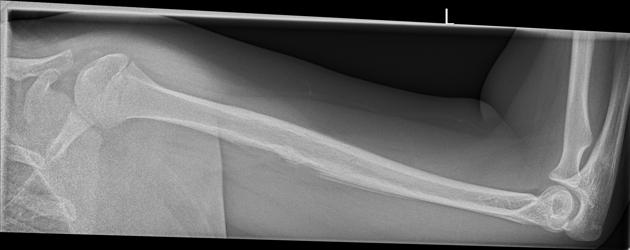
Radiography is the optimal initial imaging modality for evaluating undiagnosed primary bone tumours 1-3,7. The radiographic features of a bone lesion are often the primary determinant of non-histological diagnosis.
Essential features to describe when assessing a potentially neoplastic bone lesion include:
location in the skeleton (flat vs long bones or axial vs appendicular)
-
location within a bone
longitudinal: epiphyseal, metaphyseal or diaphyseal
transverse: medullary, eccentric, endosteal, cortical, or periosteal
morphology
size
cortical involvement
extra-osseous or soft-tissue component
CT/MRI
Advanced imaging modalities, such as CT, MRI, or nuclear medicine play a complimentary role when additional anatomic information is required for surgical planning and staging, or when clinical or radiographic features are indeterminate 2.
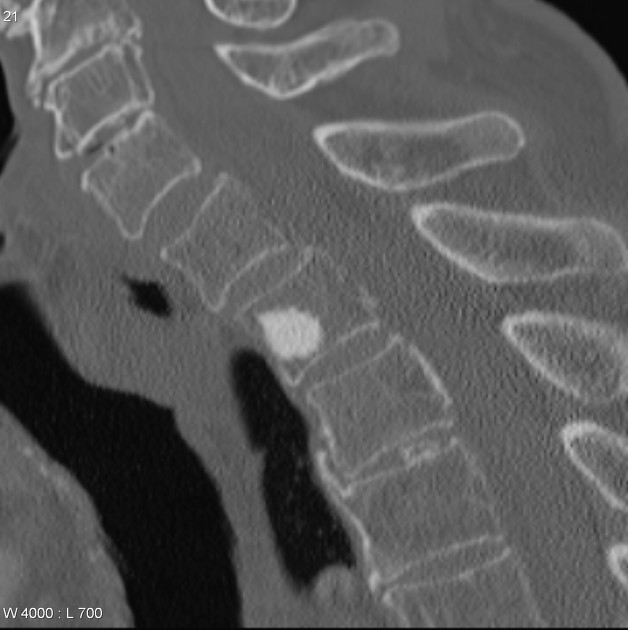
CT can enhance the ability to detect subtle matrix mineralisation or periosteal reaction that may not be seen on radiographs or MRI.
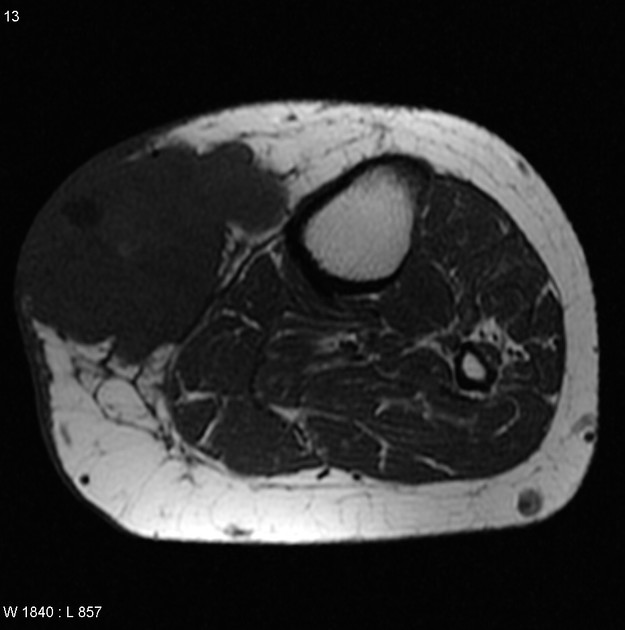
MRI provides added soft-tissue contrast, which allows for evaluation of the tissue composition (e.g. fat, haemorrhage, fluid-fluid levels) and anatomic extent of bone tumours.
Treatment and prognosis
Treatment and prognosis vary not only with stage but also with histologic type.
More indolent processes may be managed with curettage combined with local adjuvants such as bone cement (polymethyl methacrylate), bone graft, phenol or liquid nitrogen.
In general, for more aggressive lesions, surgery, chemotherapy, and radiotherapy are offered according to the stage, resectability, operability, and functional status. Targeted treatments depend on molecular testing.
Differential diagnosis
The protean differential list can be ordered in many ways and no system is perfect. Below are links that may be useful in day-to-day practice.
Patterns of matrix produced
Approximates the WHO classification described above.
-
bone-forming tumours – cumulus cloud
see: osteoid lesions
-
cartilage-forming tumours – popcorn or rings or arcs
see: chondroid lesions
-
fibrous bone tumours – ground glass
see: fibrous lesions
Pattern of location
Anatomical
Skeletal
-
head and neck
-
chest
-
spine and extremities
Patterns of morphology
lucent/lytic bone lesions (FEGNOMASHIC) (mnemonic)
expansile lytic lesions without cortical destruction of bone
bone tumours with internal trabeculations (mnemonic)
multiple lucent/lytic bone lesions (mnemonic)
benign lytic bone lesions in patients under 30 years old (mnemonic)
diffuse bony sclerosis (mnemonic)
Pattern of metastasis
bone metastases (full article)
tumours that metastasise to bone (mnemonic)



























 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}