
Bowel and mesenteric trauma can result from blunt force, penetrating and iatrogenic trauma. CT is the gold standard imaging modality but CT findings are nonspecific 12.
On this page:
Epidemiology
The bowel and mesentery are injured in ~2.5% (range 0.3-5%) of blunt force abdominal trauma 1,3,5,8. However not surprisingly, bowel and mesenteric injuries are more frequent after penetrating trauma 8. Bowel injury has consistently been found to be the most common traumatic abdominopelvic injury missed on CT 11.
Pathology
Etiology
Gunshot wounds (~75%) and stabbings (~20%) are the leading causes of bowel and mesenteric injury from penetrating trauma 8. Motor vehicle collisions are the most common cause of blunt trauma followed by falls, assaults and sports-related trauma 4,6.
Types
From most to least common sites of bowel injury 1,4,6:
jejunum (near ligament of Treitz/D-J flexure)
ileum (near ileocecal valve)
duodenum (D2 and D3 segments)
stomach (greater curvature)
The mechanism of bowel injury include crush/compression type, shearing type (from fixed point of mesentery) and burst type (from increased intra-luminal pressure) and can include 4:
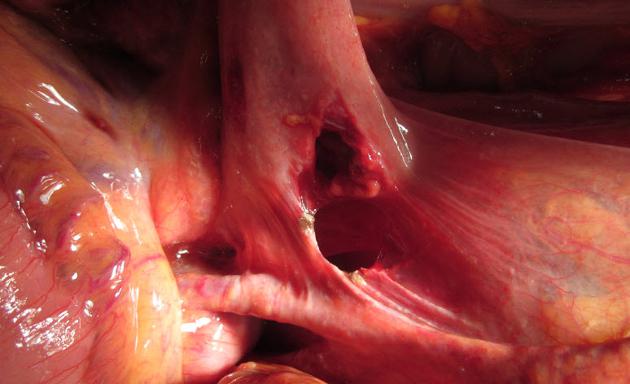
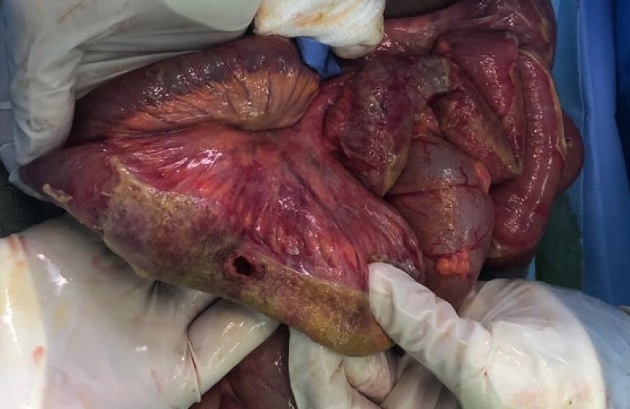
perforation
mural hematoma or edema
active hemorrhage
serosal tear
degloving (very rare)
Mesenteric injuries can include:
active bleeding from a laceration
mesenteric lacerations (e.g. bucket handle tears) which can create a site for acute or remote internal herniation of bowel
Grading schemes
Several grading schemes (RAPTOR and BIPS) using a variety of clincial parameters and CT findings have been validated and correlate with operative findings and the need for surgical intervention.
Radiographic features
Radiography
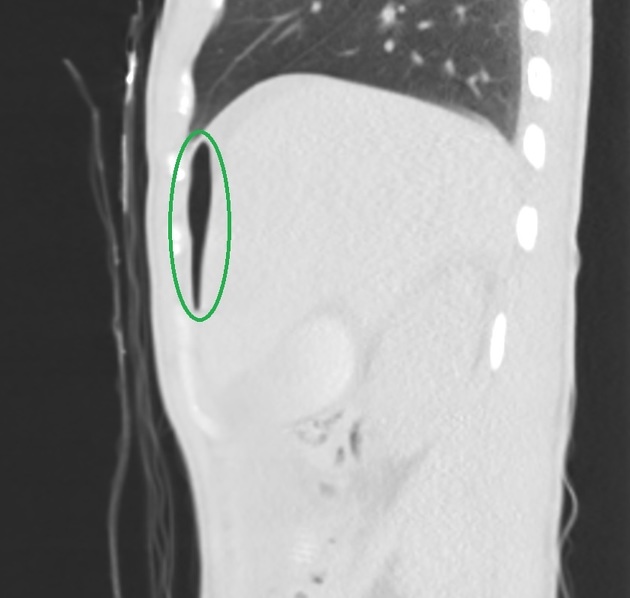
The erect chest x-ray may show free subdiaphragmatic gas due to traumatic bowel injury but radiographs indicated in the setting of trauma are almost always performed as a supine projection which reduces the sensitivity of pneumoperitoneum. Abdominal radiography is not indicated in trauma when CT is readily available.
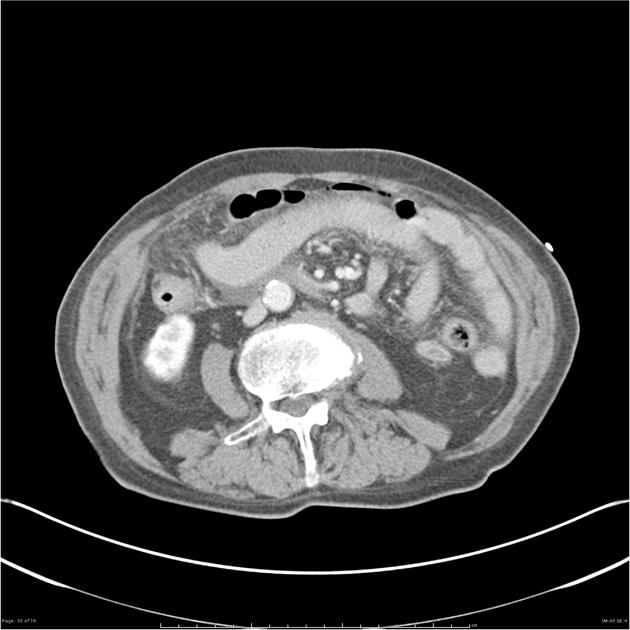
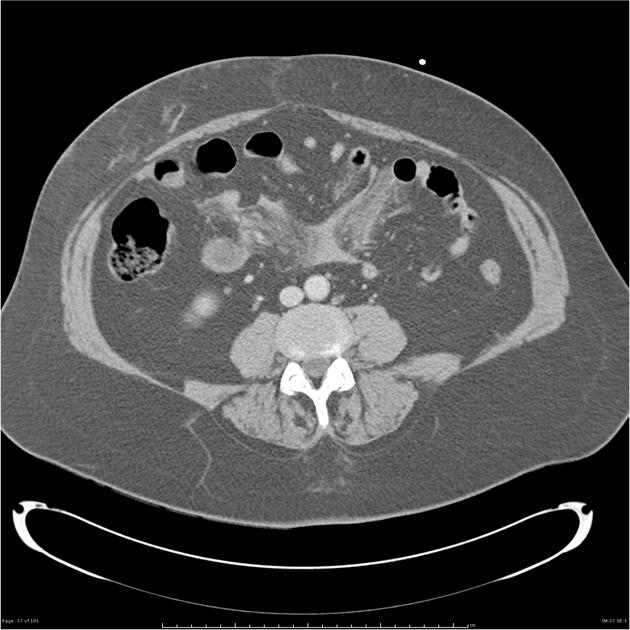
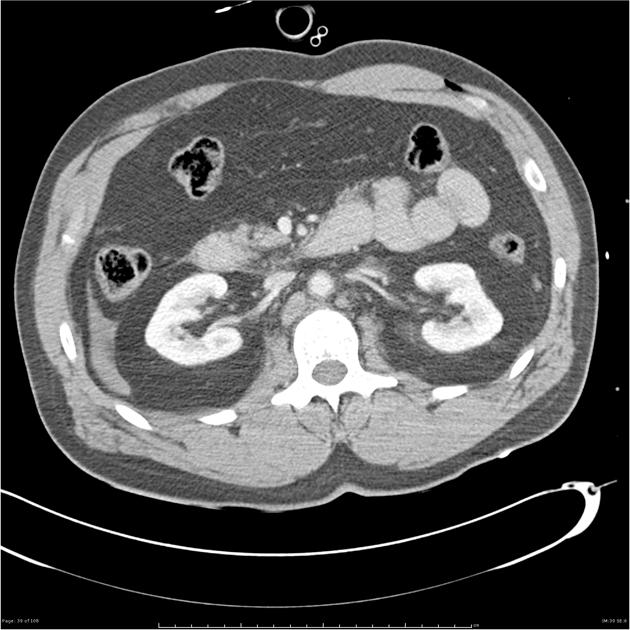
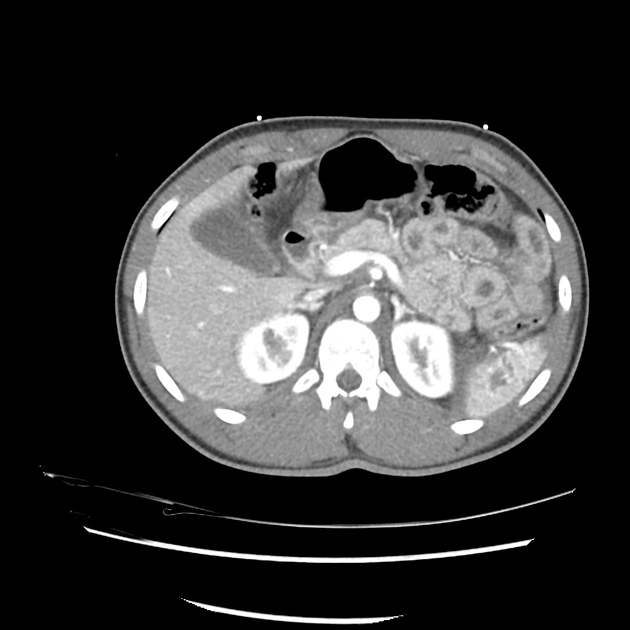
CT
Bowel injury
-
definitive signs:
visible bowel wall discontinuity 7
-
perforation
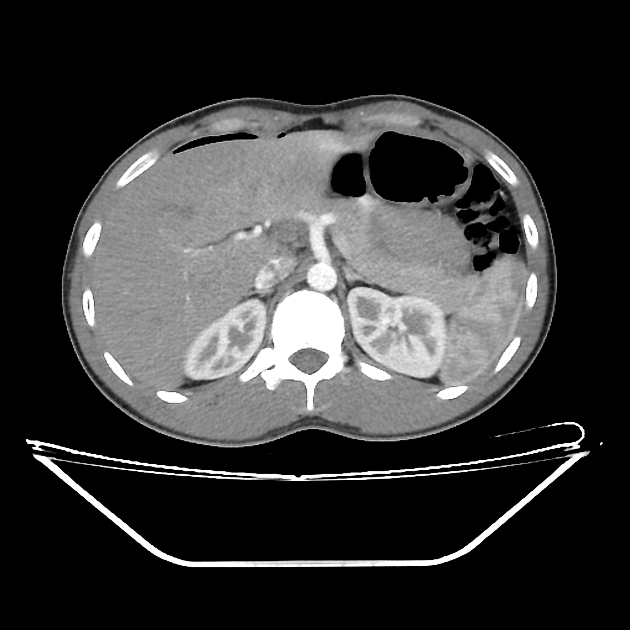
in blunt trauma, the presence of extra-luminal oral contrast media (if used) or bowel contents; extra-luminal free gas (especially in the absence of pneumothorax/pneumomediastinum) 2
in penetrating trauma, extra-luminal free gas is not specific to bowel perforation; extra-luminal contrast media/bowel contents leak and a wound track extending to bowel is considered the most sensitive; wall thickening/mesenteric contusion is less sensitive 2
-
suggestive signs 7
mural hematoma: discontinuity in the bowel wall with mural thickening (>3-4 mm); may be complete (i.e. perforated) or incomplete 2,4
moderate/large volume of free fluid without solid organ injury 2-3
intermesenteric (interloop) fluid, often forming triangles
abnormal bowel wall enhancement: decreased due to mesenteric vascular interruption and small bowel ischemia, or increased due to vascular permeability secondary to hypoperfusion 7
positive seatbelt sign increases the likelihood of traumatic bowel injuries 9
feacalisation 12
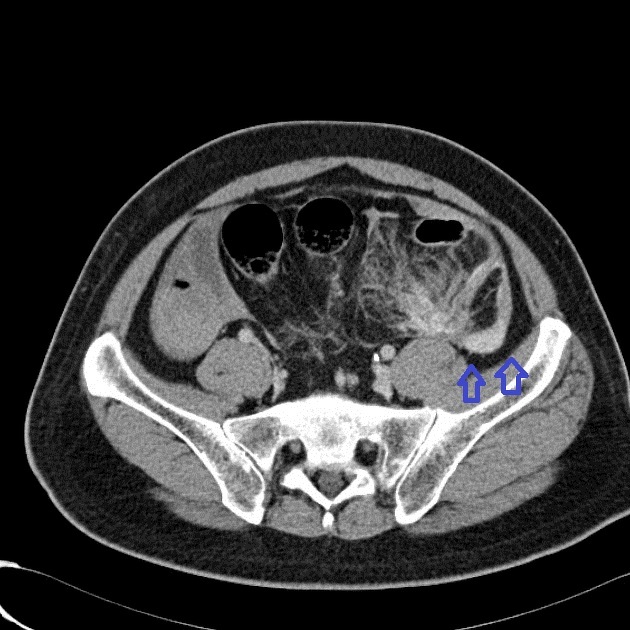
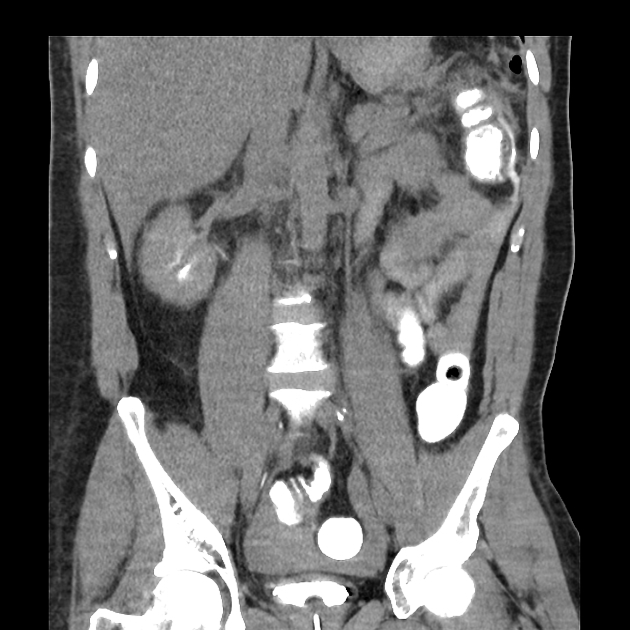
Mesenteric injury
-
definitive signs:
active extravasation of contrast media is indicative of active bleeding and a significant mesenteric injury 3
intermesenteric (interloop) free fluid, often forming triangles 7
beading and termination of mesenteric vessels 4, 7
abrupt termination of the mesenteric vessels 7
accumulation ('pooling') of contrast on multiphase imaging
-
suggestive signs 7
mesenteric infilatration: haziness and fat stranding
mesenteric hematoma
bowel wall thickening
Treatment and prognosis
Even with increasing non-operative management of traumatic abdominal organs (e.g. liver or spleen laceration), traumatic bowel and mesenteric injuries such as perforation or active mesenteric bleeding still require operative management 3.
Differential diagnosis
shock bowel: diffuse bowel wall thickening (from edema) that is hyperenhancing

















 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.