
Presentation
Motorbike rider vs. car at 180 km/hr.
Patient Data
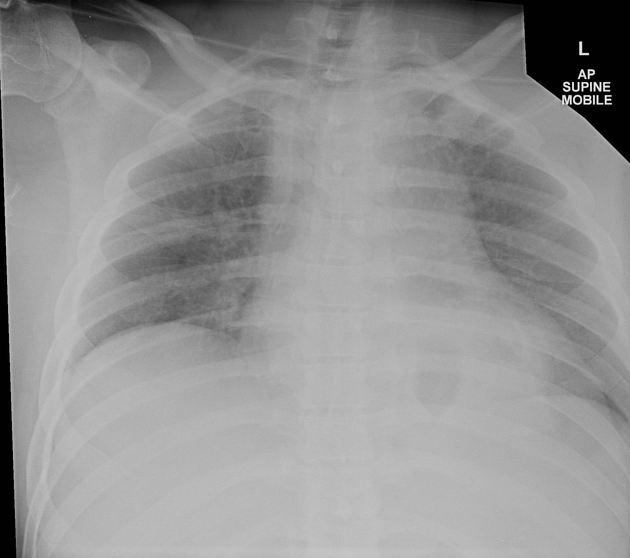
Heart size is normal. Markedly widened mediastinum. Gastric fundus lies within the left inferior chest raising the possibility of ruptured left hemidiaphragm.



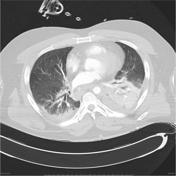
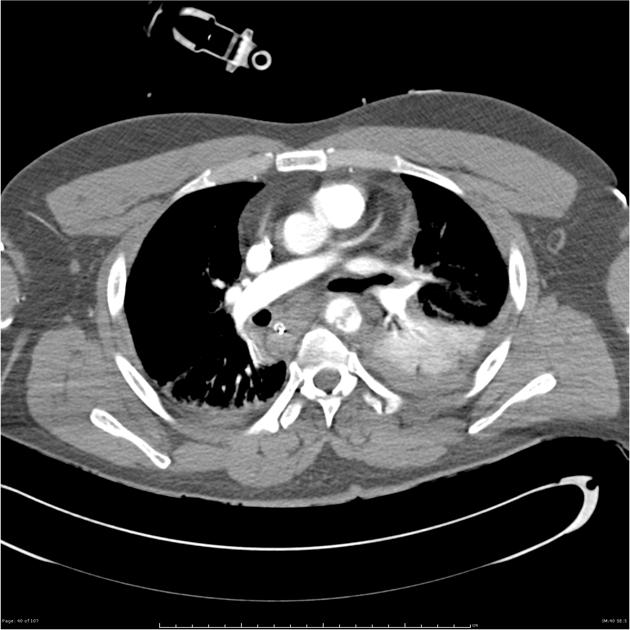
Blunt aortic injury / partial transection at the isthmus and large pseudoaneurysm. Large volume middle mediastinal hematoma with right tracheal and esophageal deviation Left diaphragmatic rupture and stomach herniation into the posterior mediastinum. Low volume brachiocephalic vessels, suggesting volume depletion. Left hemothorax, alveolar opacity compatible with pulmonary contusion, and posterior atelectasis. Small right sided pneumothorax and posterior pulmonary contusions. Displaced right posterior 12 rib fracture. No scapular or sternal fracture.


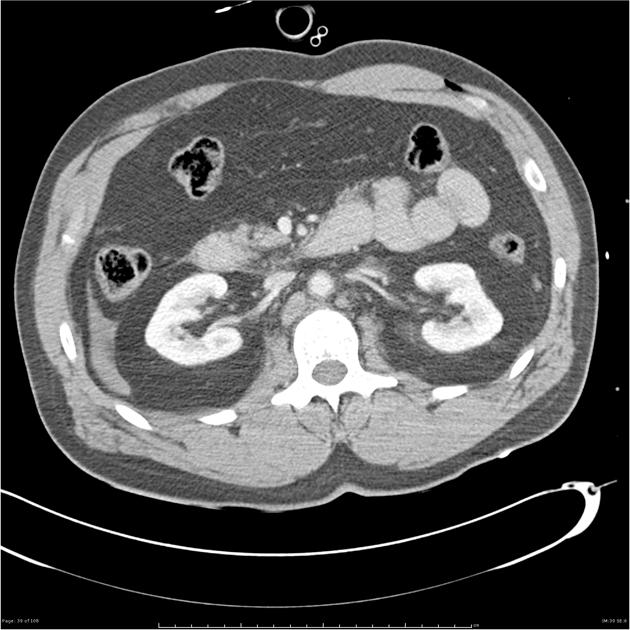
Left diaphragmatic rupture with stomach herniation. Moderate volume hemoperitoneum. 2 cm subcapsular splenic contusion without a large localized splenic hematoma. Fat stranding surrounding the D3 and D4 duodenal segments and significant proximal jejunal wall thickening consistent with blunt duodenal and jejunal injury. Small bowel mesenteric fat stranding suspicious for a mesenteric tear. No arterial contrast extravasation detected. Focal right lower renal pole poorly defined cortical hypodensity, possibly a blunt renal contusion. "Flat" or low volume IVC consistent with volume depletion. Extensive soft tissue gas detecting superiorly from the facial planes in both thighs into the adductor fat planes in the anterior abdominal wall, likely related to the open femoral injuries.
Case Discussion
In summary, injuries sustained:
- traumatic thoracic aorta injury (treated with stent-graft)
- hemothorax
- pneumothorax
- pulmonary contusion
- diaphragmatic rupture
- splenic contusion
- bowel and mesenteric injury (jejunal tear confirmed at surgery - small bowel resection)


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.