
CT guided percutaneous drainage is one form of image-guided drainage, allowing minimally invasive treatment of collections, potentially anywhere in the body. Although less commonly used than ultrasound guidance, it is particularly valuable in gaining access to deeper or more posterior parts of the body.
It has several advantages and disadvantages over ultrasound, which include:
-
advantages
can safely access areas not well visualised on ultrasound
vision is not obscured by gas
better vision in larger patients
is less user-dependent for those less confident with ultrasound-guided procedures
the CT table in some ways offers more stable positioning for the patient
in the intubated patient it allows for better monitoring and positioning of equipment
-
disadvantages
is not truly dynamic like ultrasound, although CT fluoroscopy does allow near-immediate imaging
exposes the patient to ionising radiation
requires a wider range of staff to undertake compared to ultrasound
harder in the uncooperative patient as movement, means access point lost
Procedure
Pre-procedure evaluation
Laboratory results
Interventional procedures like percutaneous drainage require special attention to coagulation indices. The values suggested below were considered based on the literature review, whose references are cited below:
-
complete blood count
platelet >50000/mm3 (some institutions determine other values between 50000-100000/mm3) 2
-
coagulation profile
international normalised ratio (INR) ≤1.5 2
normal prothrombin time (PT), partial thromboplastin time (PTT)
some studies showed that having a normal INR or prothrombin time is no reassurance that the patient will not bleed after the procedure 3
Imaging
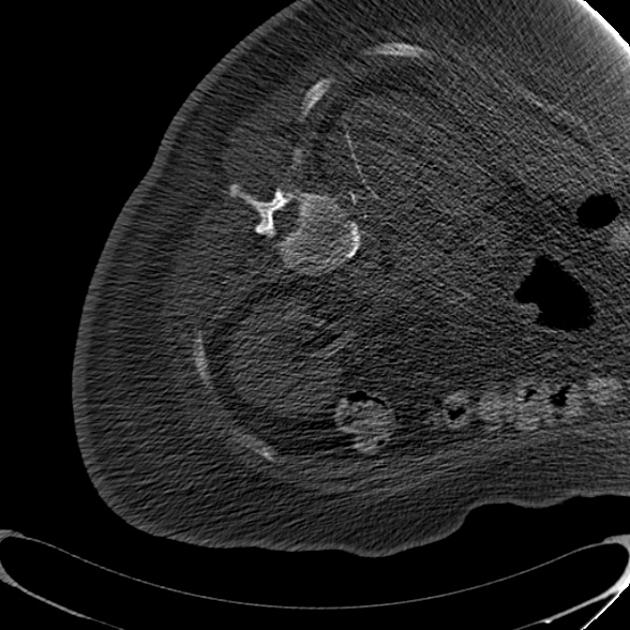
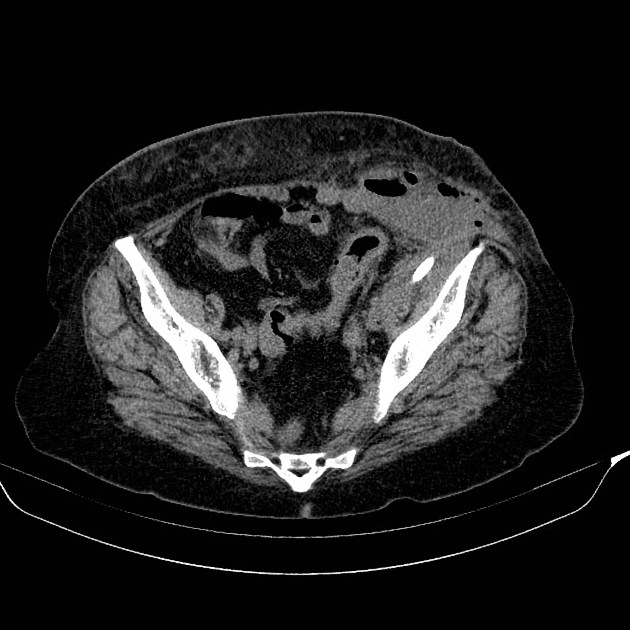
Review the diagnostic CT and other relevant imaging first to clarify the collection that is requested to be drained, and the shortest possible route without traversing important structures 1.
In some selected cases other anatomical structures are purposely traversed as part of the treatment, such as the stomach when undertaking pancreatic pseudocyst drainage.
Technique
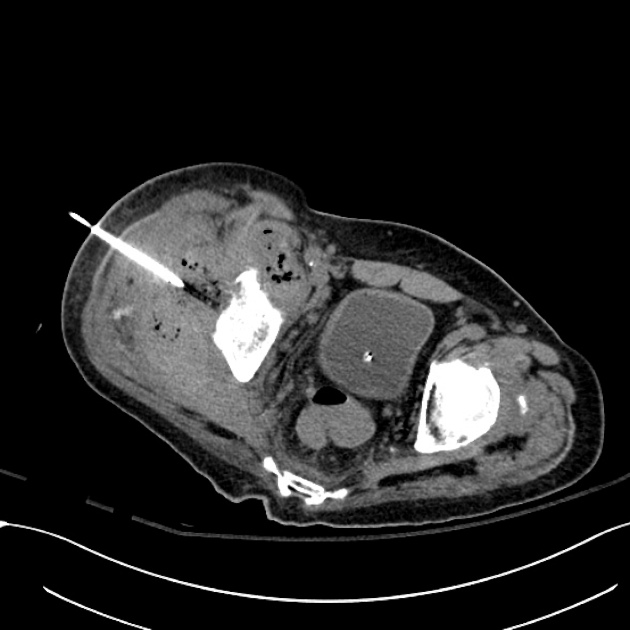
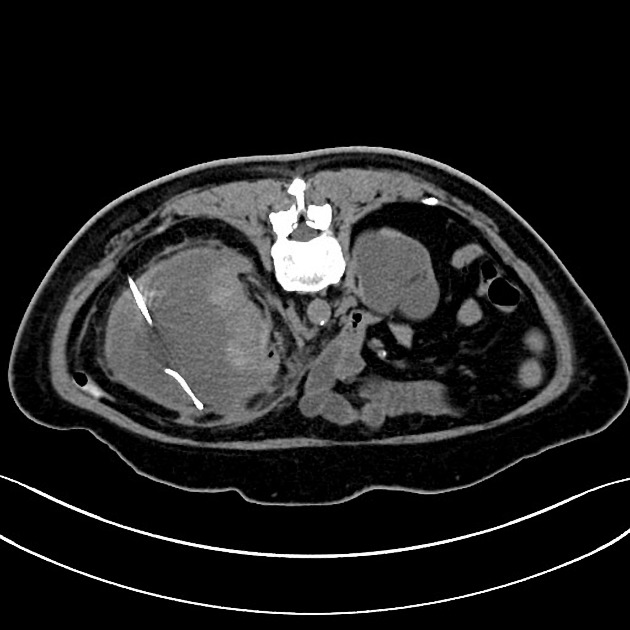
The technique is largely the same as for ultrasound-guided percutaneous drainage procedures, with either a single step or multistep technique, although the latter is more commonly used in CT. A two- or three-part access needle is used to enter the abscess/collection, followed by the use of a stiff wire and serial dilators, before a catheter is placed.
The catheter is then connected to a vacuum drainage system (for peritoneal or retroperitoneal space collections) or external drainage bags (for draining urinary, digestive and biliary tracts).
Post-procedure care
The patient's basic observations should be monitored for four hours (i.e. pulse, BP, SpO2).
The patient should remain in bed for two hours. After this mobilisation is permissible as is being able to eat and drink.
The entry site should be reviewed on a daily basis. Once the output from the collection ceases, repeat imaging should be considered before removing the drainage catheter.








 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.