
The renal mass CT protocol is a multiphasic contrast-enhanced examination for the assessment of renal masses. It is most often comprised of a non-contrast, nephrogenic phase and excretory phase. However, this article will cover the optional, corticomedullary phase too.
NB: This article is intended to outline some general principles of protocol design. The specifics will vary depending on CT hardware and software, radiologists' and referrers' preference, institutional protocols, patient factors (e.g. allergy) and time constraints.
On this page:
Terminology
For some departments and/or radiologists, a renal mass protocol may only include a non-contrast, nephrogenic phase exam. For others, it may consist of a corticomedullary phase (40-60 second delay) and/or an excretory phase (5-10 minute delay).
Indications
Indeterminate renal mass, renal adenocarcinoma, metastasis, monitoring of known renal mass.
Purpose
The purpose of this exam is to assess the location and composition of a renal mass.
non-contrast scan is best to determine the HU of homogenous renal mass or masses containing macroscopic fat 1
corticomedullary phase is best to delineate subcategories of renal cell carcinomas further
nephrogenic phase is best for optimal enhancement of the renal parenchyma, including the renal medulla, and will demonstrate enhancing components of a mass
excretory phase will demonstrate enhancement of calyces, renal pelvis and ureters. Many institutions will perform this around 5 minutes to demonstrate opacification of the ureters
Technique (4 phase)
-
patient position
supine with their arms above their head
-
scout
diaphragm to the lesser trochanter
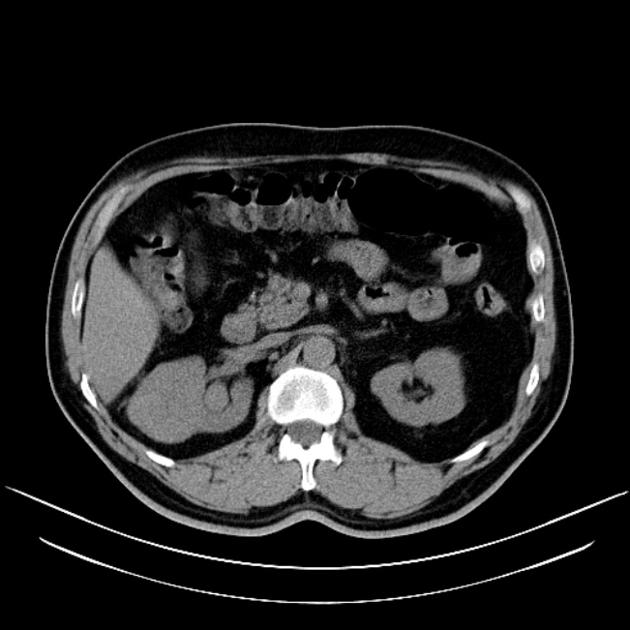
Non-contrast scan
-
scan extent
mid-diaphragm to the iliac crest (covering kidneys)
-
scan direction
craniocaudal
-
scan delay
none
-
respiration phase
inspiration, breath-hold
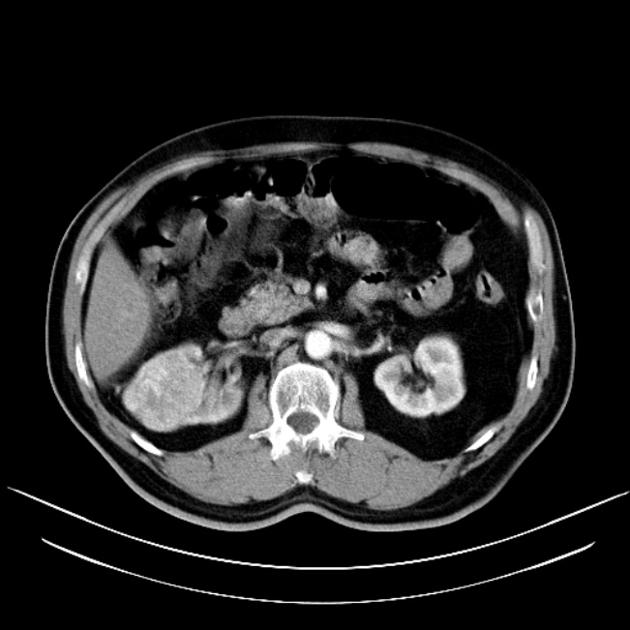
Corticomedullary phase
-
scan extent
mid-diaphragm to the iliac crest (covering kidneys)
-
scan direction
craniocaudal
-
contrast injection considerations (bolus tracking)
-
monitoring slice (region of interest)
level of the diaphragmatic hiatus or first lumbar vertebra at the aorta
-
-
threshold
150 HU
-
volume
100 mL of non-ionic contrast at 3 to 5 mL/s (a higher flow rate will equal greater enhancement)
-
scan delay 2
-
corticomedullary
20-30 seconds post bolus trigger (30-40 s after injection)
-
-
respiration phase
inspiration, breath-hold
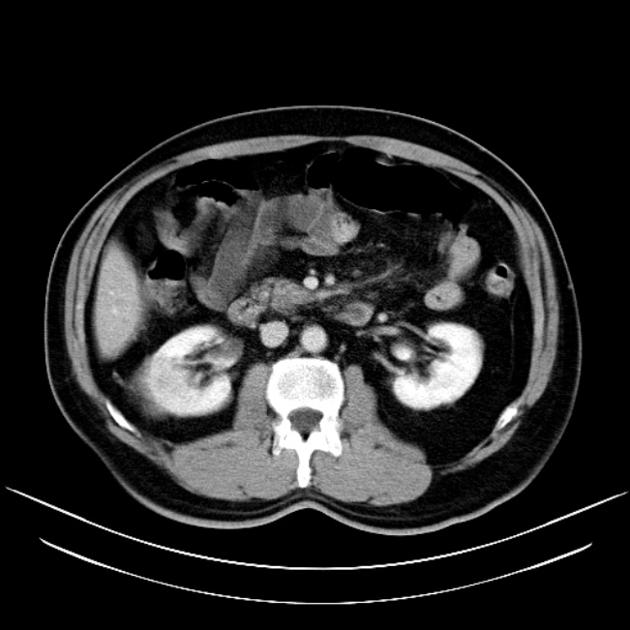
Nephrogenic phase
-
scan extent
mid-diaphragm to lesser trochanter (covering entire renal system)
-
scan direction
contrast injection considerations
-
scan delay
-
nephrographic phase
100 seconds post-injection
-
-
respiration phase
inspiration, breath-hold
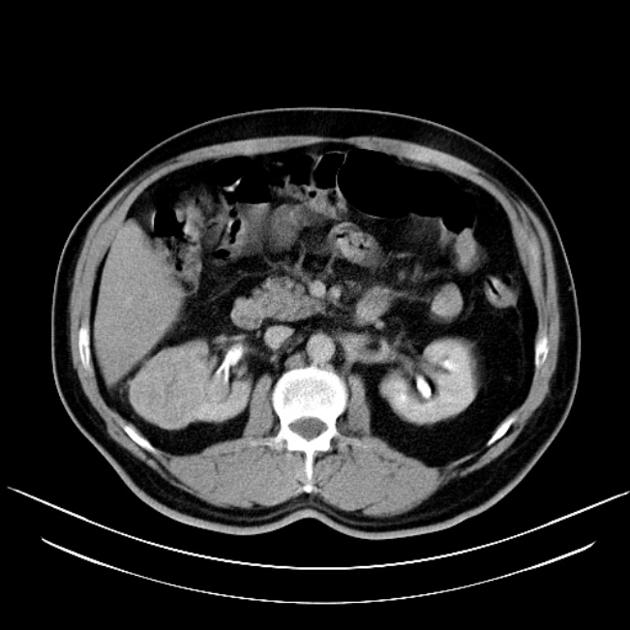
Excretory phase
-
scan extent
mid-diaphragm to lesser trochanter (covering entire renal system)
-
scan direction
craniocaudal
contrast injection considerations
-
scan delay
-
excretory phase
5-10 minutes post-injection
-
-
respiration phase
inspiration, breath-hold
Practical points
pseudoenhancement, an artifact encountered where the calculated density of a lesion is inaccurately increased, is a problem often noted in renal mass scans, dual-energy CT via virtual monoenergetic images at a KeV range of 80 Kev to 90 KeV can minimise beam hardening and partial voluming and overcome this issue


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.