
Dilated cardiomyopathy (DCM) is defined as left ventricular chamber dilation with global or regional systolic dysfunction not sufficiently explained by abnormal loading conditions (such as valvular heart disease, congenital heart disease, hypertension etc.) or coronary artery disease 1-4.
It might be associated with right ventricular dysfunction. Causes are related to intrinsic myocardial damage.
On this page:
Clinical presentation
Presenting symptoms are nonspecific and are secondary to elevated venous filling pressures as well as decreased end-organ perfusion secondary to a progressive decrease in cardiac output:
-
dyspnoea
exacerbated by supination, bending forward at the waist, and exertion
fatigue, early satiety, cough
peripheral oedema
Physical examination is likewise nonspecific but may reveal a laterally displaced apical impulse, auscultatory S3, jugular venous distension, dependent auscultatory crackles in the basilar lung segments, and pitting-dependent peripheral oedema.
Pathology
The ventricles are dilated and poorly contractile with normal or reduced wall thickness. The atria may also have a similar appearance and function.
Aetiology
Although a variety of aetiologies can result in dilated cardiomyopathy which are listed below. Some are classified as separate entities. (See WHO 1995 classification of cardiomyopathies)
-
infectious (myocarditis)
viral (e.g. coxsackievirus, echovirus, adenovirus)
bacterial (e.g. diphtheria, mycoplasma, listeria)
-
infiltrative disease
-
endocrine/metabolic derangements
uraemia, hypocalcaemia, hypophosphataemia
thyrotoxicosis, thiamine deficiency (i.e. "wet" beriberi)
-
toxic
-
chemotherapy
anthracyclines (e.g. doxorubicin, daunorubicin)
mitoxantrone
checkpoint inhibitors
-
others
-
autoimmune
late-onset cardiomyopathy in Chagas disease
-
idiopathic
-
familial
Associations
Radiographic features
Plain radiograph
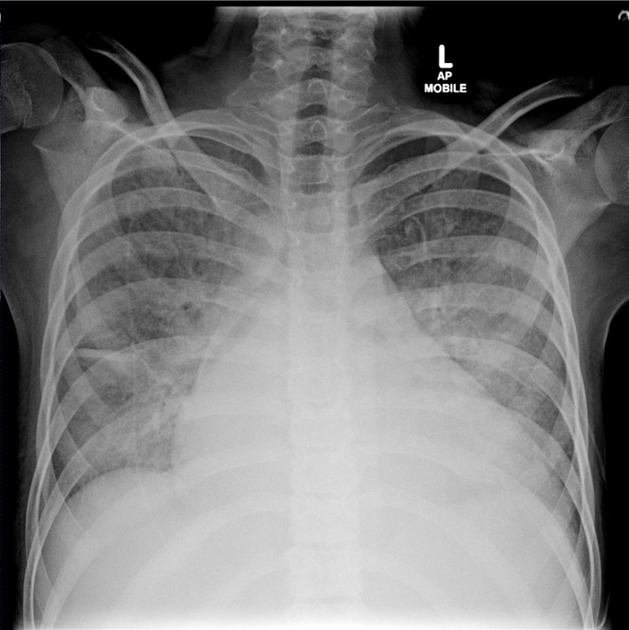
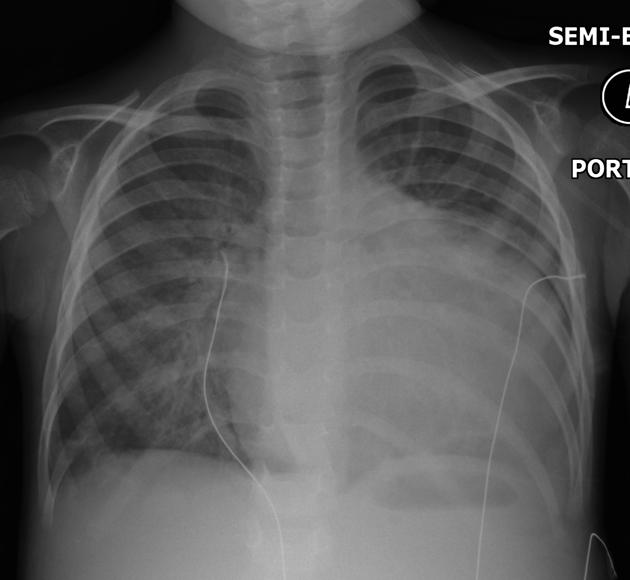
Chest radiographs commonly show an enlarged left ventricle and atria with pulmonary oedema. Associated pleural effusions may also be seen.
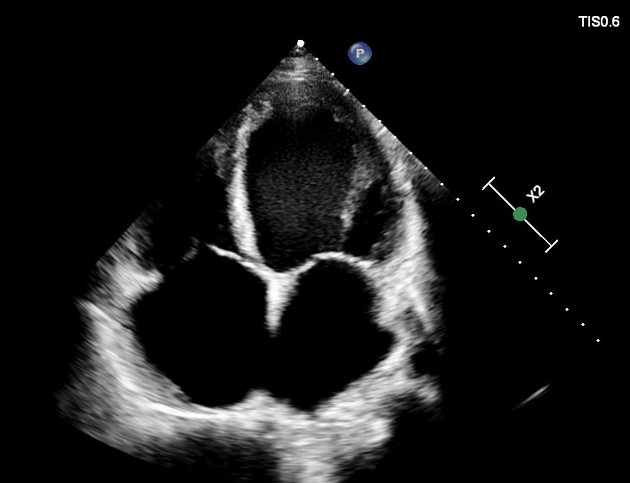
Ultrasound: echocardiography
The degree of left ventricular dilatation is highly variable and depends on the stage of disease and severity of left ventricular dysfunction.
-
global ventricular chamber dilation
-
elevation in left ventricular mass and volumes
may be inferred by an LV end-diastolic diameter above 5.9 cm (males) or 5.3 cm (females)
ventricular wall thickness may be normal or reduced (<0.6 cm)
-
ventricle may appear spherical with a decreasing length: width ratio
normal left ventricular long: short axis ratio ~1.5
-
-
secondary mitral regurgitation
mitral annular dilation, failure of leaflet coaptation, stretching of subvalvular apparatus
-
systolic dysfunction
left ventricular ejection fraction will decrease, with a normal or reduced stroke volume
-
left atrial dilation implies a degree of chronicity
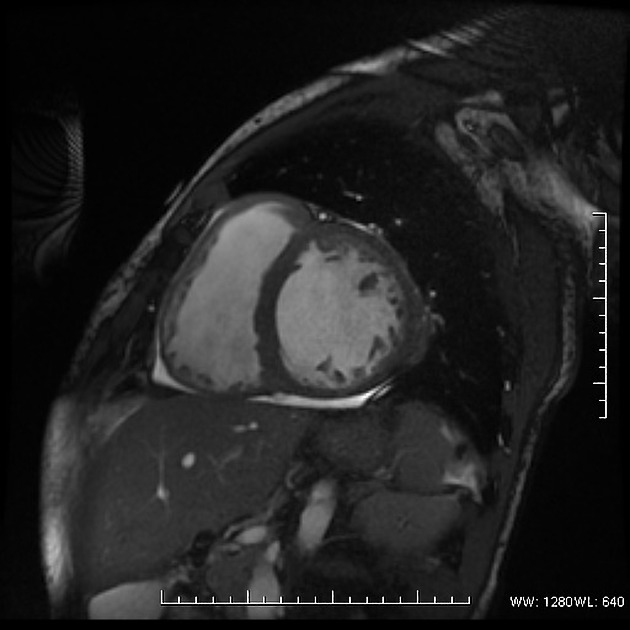
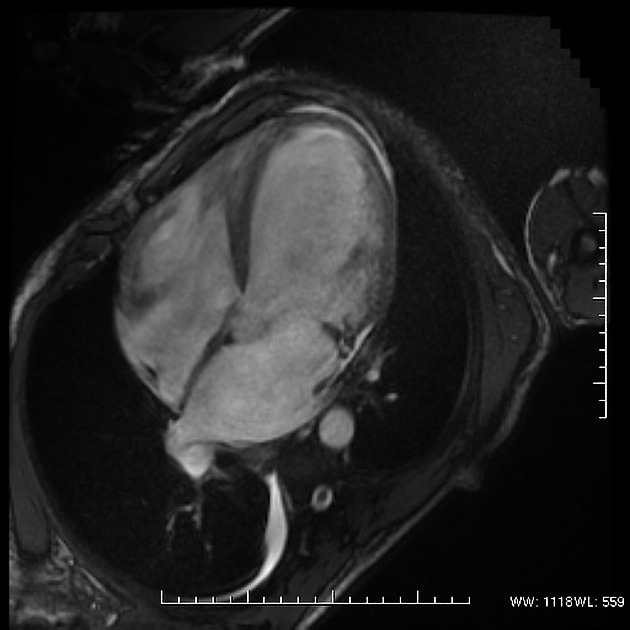
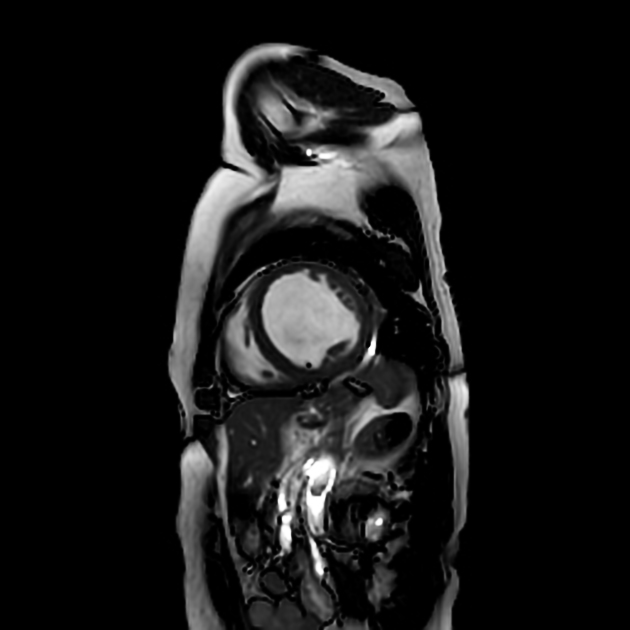
MRI
In idiopathic dilated cardiomyopathy, the left heart is markedly dilated and thinned, and mid-wall enhancement, especially in the septum, is present in more than 50% of patients 6.
Late enhancement MR images may demonstrate areas of fibrosis within the myocardium, characteristically in the mid- or subepicardial myocardium, allowing differentiation from ischaemic cardiomyopathy 5.
Differential diagnosis
Conditions mimicking the clinical presentation or imaging appearance of dilated cardiomyopathy include:
ischaemic cardiomyopathy/left ventricular aneurysm
left ventricular dilatation due to valvular heart disease
On plain radiographs consider:
large pericardial effusion





 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.