
Dupuytren contracture, also called Viking disease, or palmar fibromatosis, is a fibrosing condition that characteristically presents as a firm nodularity on the palmar surface of the hand with coalescing cords of soft tissue on the webs and digits.
On this page:
Epidemiology
Dupuytren contracture is considered the most common of the superficial fibromatoses. Prevalence is estimated at 1-2% of the population 12, increasing to 20% at the age of 65 years. There is a male predominance (~3.5:1 M:F) 12.
People of northern European descent are typically affected with the highest prevalence in countries such as northern Scotland, Iceland, Norway and Australia 2.
Clinical presentation
Patients typically present with palmar surface subcutaneous nodules on the distal crease of the hand. This may progress to cords and bands and finally, the characteristic flexion contracture secondary to fibrous attachments to the underlying tendon sheath.
Pathology
Dupuytren contracture is a progressive condition that causes shortening and thickening of the fibrous tissue of the palmar fascia.
Location
lesions can be bilateral in about half of cases 7,12
the 4th ray is typically involved 6
Associations
Additional diseases that are associated with palmar fibromatosis include:
phenobarbital treatment of epilepsy 12
alcohol use 12 (particularly liver disease related to alcohol use ref)
repeated vibrational trauma 12
keloids ref
-
other fibromatosies
plantar fibromatosis: co-occurs in ~10% of patients 12
Peyronie disease: co-occurs in ~2.5% (range 1-4%) of patients 12
knuckle pads 13
Radiographic features
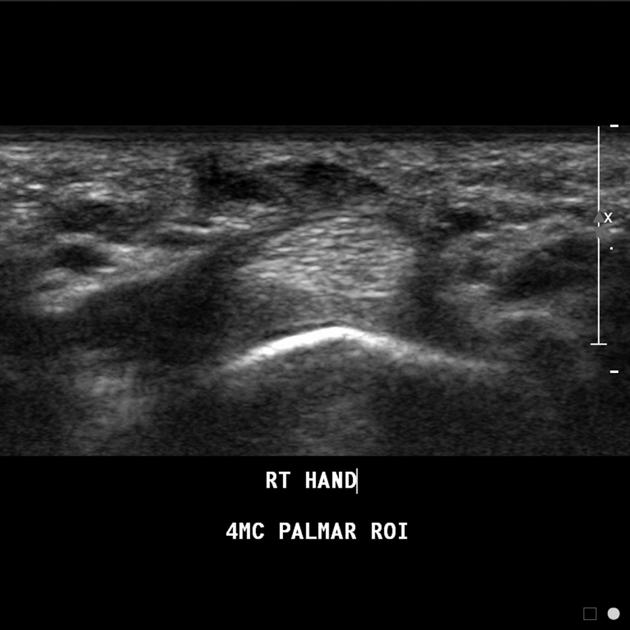
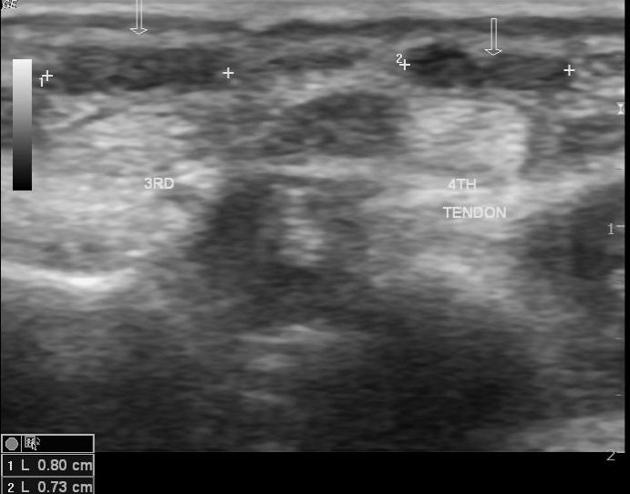
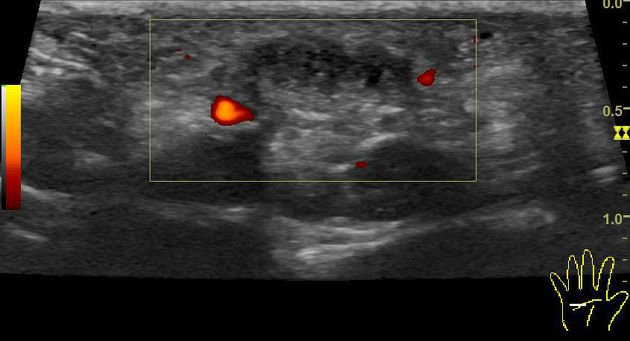
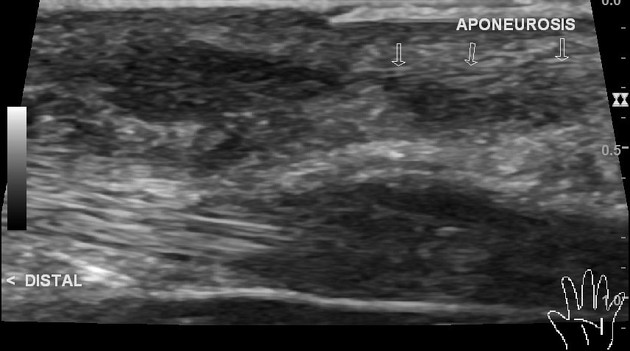
Ultrasound
Initial findings are of nodules seen superficial to the flexor tendons in the superficial fascia of the palm. Early on these appear hypoechoic to tendons with hypervascularity while chronic nodules can appear hyperechoic without associated vascularity 9. These can progress to hypoechoic cords and bands adhering to the flexor tendon margins, eventually resulting in the characteristic clinically apparent contracture deformity.
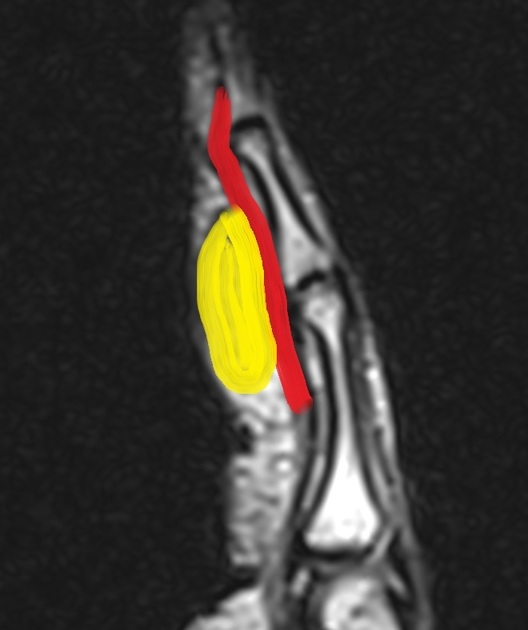
MRI
The lesions typically comprise of subcutaneous nodules, usually at the level of the distal palmar crease and cords that lie parallel and superficial to the flexor tendons.
Signal characteristics
Typical (~80% of cases) 1
T1: uniformly low signal intensity (similar to the signal intensity of tendon)
T2: uniformly low signal intensity (similar to the signal intensity of tendon)
Atypical 1
T1: low to intermediate signal intensity (a slightly higher signal intensity than that of the tendon)
T2: low signal intensity
Treatment and prognosis
Medical or surgical intervention may be required in patients suffering from a functional impairment (significant inability to use their hands for routine activities) or due to cosmetic embarrassment. Medical intervention includes triamcinolone, lidocaine or collagenase injection. Vitamin E, gamma interferon, dimethyl sulfoxide and splinting are not considered adequate treatments for Dupuytren contracture. Surgical release of palmar fascia is usually indicated in patients with severe functional impairment and neurovascular deficit in a finger 8.
History and etymology
This condition was originally described in 1831 by the French anatomist and military surgeon, Baron Guillaume Dupuytren (1777-1835) 2.
Differential diagnosis
As a general differential for contracted fingers, consider other forms of contractures such as
-
congenital contractures
neurological pathology
arthrogryposis: tends to be quite severe and involve the hand as well
-
acquired contractures


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.