
Hibernomas are rare benign fatty tumors that arise from the vestiges of fetal brown fat and are named “hibernoma” because they resemble brown fat in hibernating animals 1.
On this page:
Epidemiology
Hibernomas occur in a wide age range (from 2-75 years) 2,3, but are most often found in young adults between the ages of 20 and 40 and are slightly more common in males 2,3. They make up for about 1% of all adipocytic tumors <2% of benign fatty neoplasms 2,4.
Associations
Diagnosis
The diagnosis of hibernoma is based on histology.
Diagnostic criteria
Diagnostic criteria according to WHO classification of soft tissue and bone tumors (5th edition) 2:
multivacuolated brown fat cells
small normochromic central nuclei
Clinical presentation
They grow slowly and usually present with painless mass effect 4. Symptoms related to the compression of adjacent structures rarely develop.
Pathology
Hibernomas are tumors composed of variable amounts of brown fat cells mixed with normal white adipocytes 2-5 and are usually seen in locations where normal brown adipose tissue is present.
Etiology
There is a causative connection to multiple endocrine neoplasia type 1 2.
Location
Hibernomas are most often found in the following locations, less than 20% are intramuscular 2,3:
thigh
trunk
upper extremity
head and neck
Rare locations include 2:
abdominal cavity
retroperitoneum
thoracic
They might involve the bone very rarely, and then usually affect the axial skeleton 2,6.
Macroscopic appearance
Hibernomas are typically fatty, hypervascular lesions that are grossly similar to a lipoma. They are well-defined, encapsulated, and mobile masses. Their color varies from yellow-tan to red-brown, depending on the amount of intracellular lipid 2,3. The diameter usually ranges from 5-10 cm, but they may reach up to 20 cm or more 2,3, particularly in the retroperitoneum.
Microscopic appearance
Upon microscopic examination, the tumors are characterized by the following 1-4:
multivacuolated brown fat cells with granular eosinophilic cytoplasm and small round central nuclei
variable number of univacuolated white adipocytes
rich capillary network
no nuclear atypia, mitotic activity
focal necrosis is unusual 4
Morphologic variants of hibernoma in descending order of frequency are 1-4
typical or classical (most common): <70% brown fat content
myxoid: loose basophilic or myxoid matrix
lipoma-like: containing more univacuolated white fat cells
spindle cell: resembling spindle cell lipoma
Immunophenotype
Immunohistochemistry displays reactivity of S100 in a majority of cases 3,4. CD34 will be positive in hibernomas with spindle cell morphology 3,4. They also express the brown fat marker gene UCP1 2.
Genetics
Cytogenic abnormalities of hibernomas are 11q13 translocations affecting the tumor suppressor genes MEN1 and AIP 2,4. Those rearrangements can aid in the diagnosis and the differentiation of hibernoma over other differentials such as liposarcoma 7.
Radiographic features
Ultrasound
Appearances have been described as heterogeneous hyperechoic lesions with prominent vessels 8.
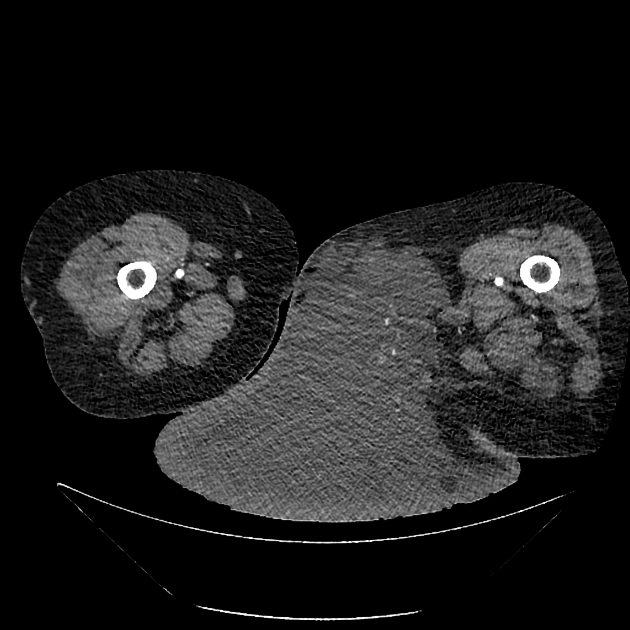
CT
On CT, hibernomas are well-circumscribed and may have a peripheral soft tissue attenuation capsule. Their attenuation varies between that of fat and skeletal muscle 8.
After contrast administration, they enhance slightly and may have prominent visible vessels 8.
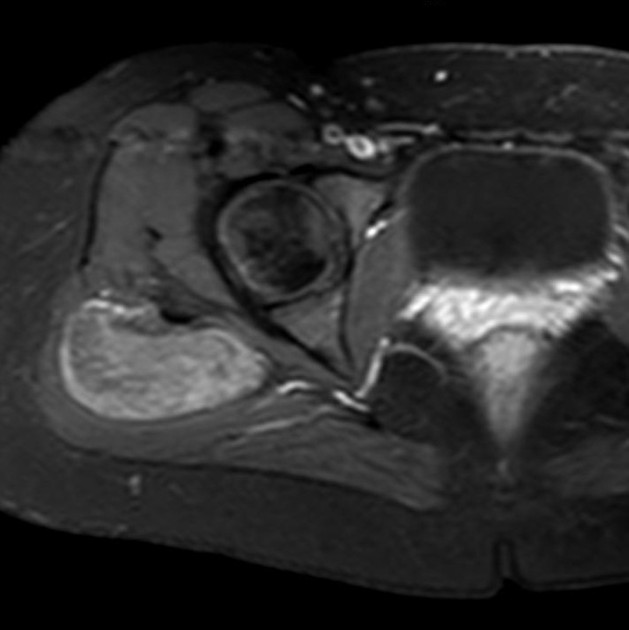
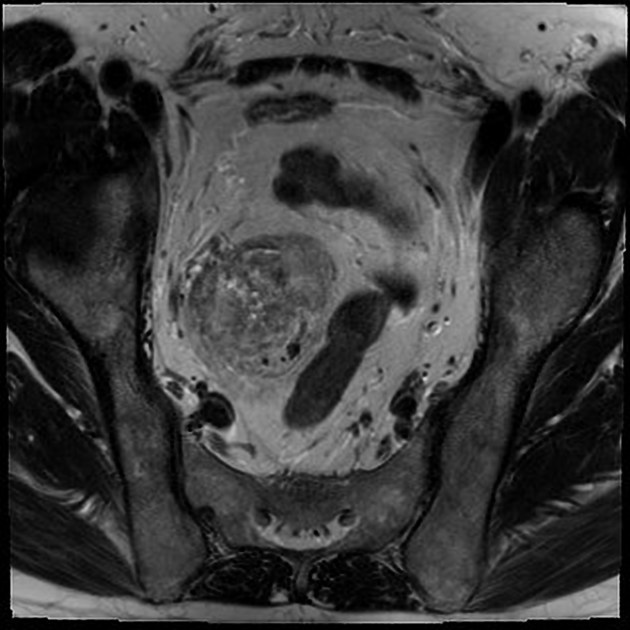
MRI
Hibernomas demonstrate high signal intensity usually slightly less than that of the subcutaneous fat also dependent on the histomorphological subtype 9. Lipoma-like hibernomas will have appearances closer to subcutaneous fat, myxoid lesions will have more fluid signal intensity whereas spindle cell hibernomas will have probably more heterogeneous areas.
All types display internal curvilinear branching septations and structures representing fibrovascular or fibrous tissue as well as flow voids indicating internal vessels 1,8-11.
There is only partial or incomplete signal loss on On fat suppression sequences due to the heterogeneous content of the mass and relatively decreased amount of lipid compared with adipose tissue 1,8.
Signal characteristics
T1: hypointense to subcutaneous fat and hyperintense to muscle
T2: usually hypointense to subcutaneous fat
STIR/T2FS/IMFS: incomplete fat suppression
T1 C+ (Gd): diffuse enhancement
Nuclear medicine
On 18FDG-PET hibernomas are FDG avid 8, although practically this has not been shown to help differentiate from malignancy
Radiology report
The radiological report should include a description of the following:
form, location and size
tumor margins and transition zone
relations to the muscular fascia
relation to neurovascular structures
Treatment and prognosis
The treatment of hibernomas consists of complete surgical excision. Local recurrence does not occur and they follow a benign course with no reported cases of metastases or malignant transformation 1-3.
History and etymology
Hibernomas were first described under the name ‘pseudolipoma’ by the German physician H. Merkel in 1906 12 and the term hibernoma was proposed by the french anatomist Louis Gery in 1914 3-5,13.
Differential diagnosis
General imaging considerations include:
resolving hematoma / Morel-Lavallée lesion



 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.