
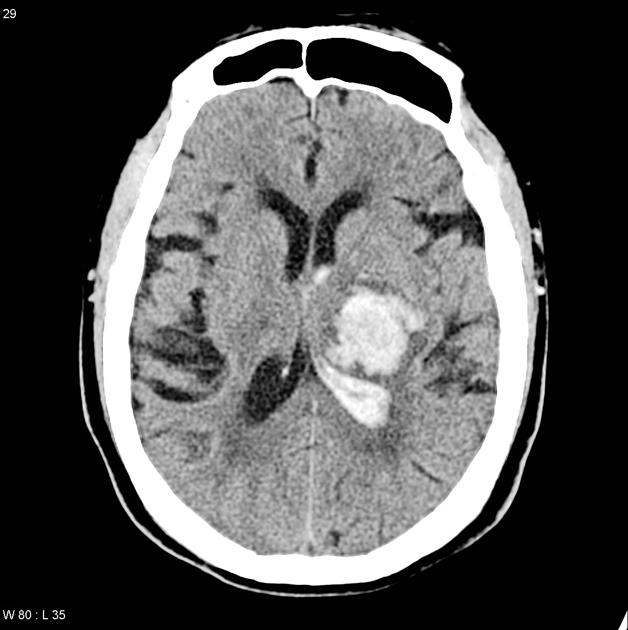
Hypertensive intracerebral haemorrhages are the most common type of intracerebral haemorrhage (ICH) by cause, commonly affecting the basal ganglia, thalamus, pons or cerebellum.
On this page:
Epidemiology
Hypertension is the single most important risk factor for ICH, with hypertensive patients 3.5x more likely to have ICH than non-hypertensive patients 5. Globally, uncontrolled hypertension accounts for ~75% of the risk for ICH 7.
Clinical presentation
Patients will present variably depending on the region and size of the haemorrhage:
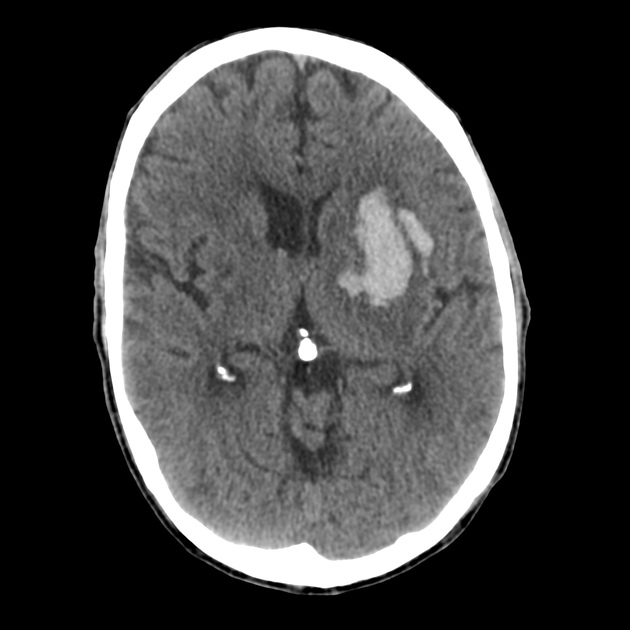
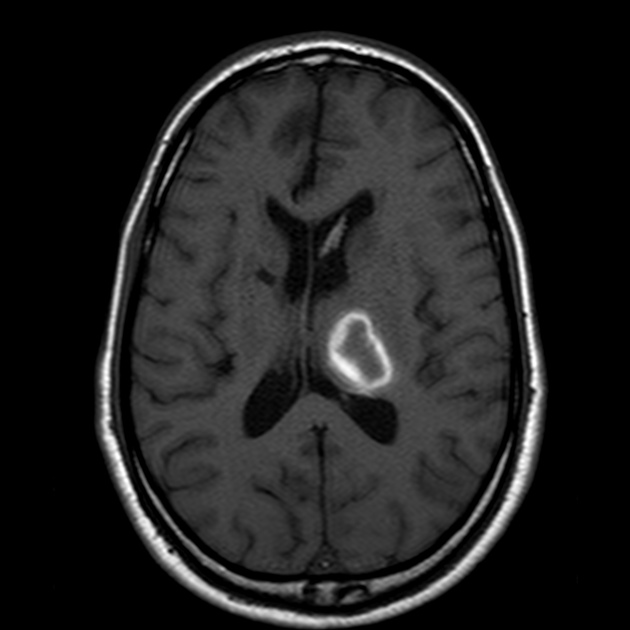
basal ganglia haemorrhage usually present with a clinical syndrome mimicking deficits from a lacunar stroke syndrome
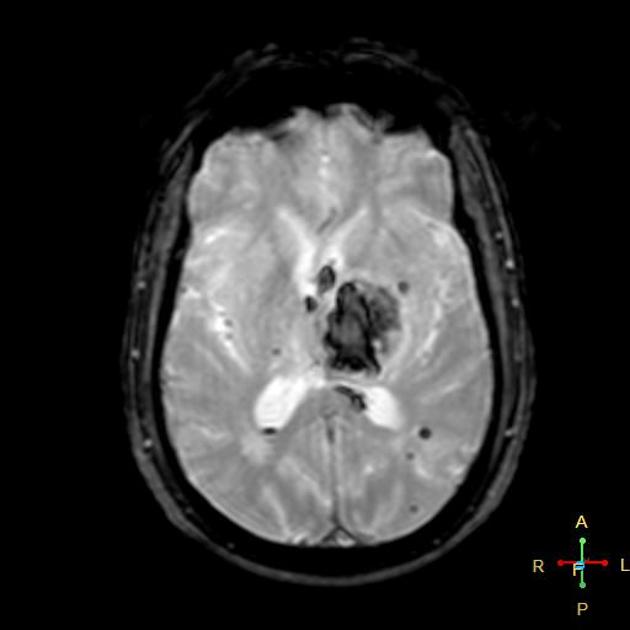
thalamic haemorrhage can have a highly varied clinical presentation depending on the exact location of the haemorrhage
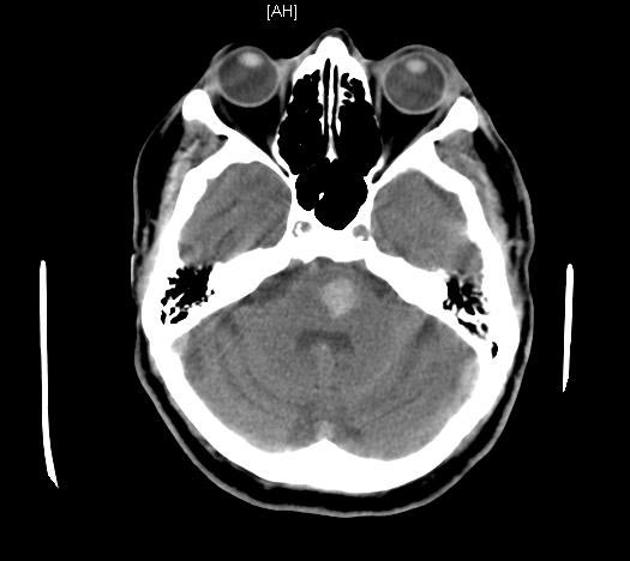
pontine haemorrhage often causes coma due to disruption of the reticular activating system (unless small) and quadriparesis due to disruption of the corticospinal tracts 4
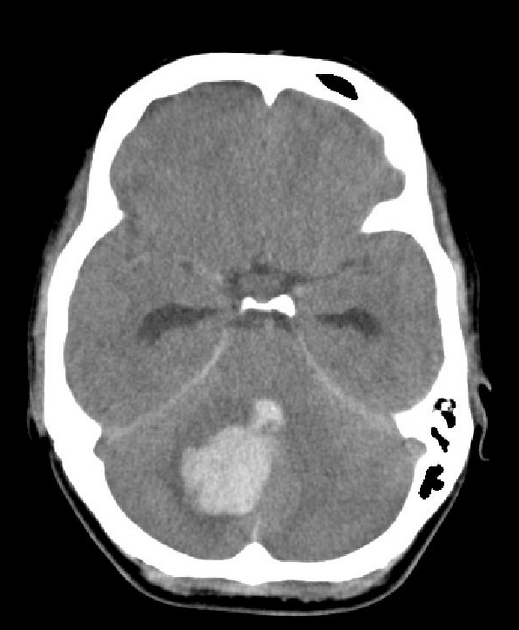
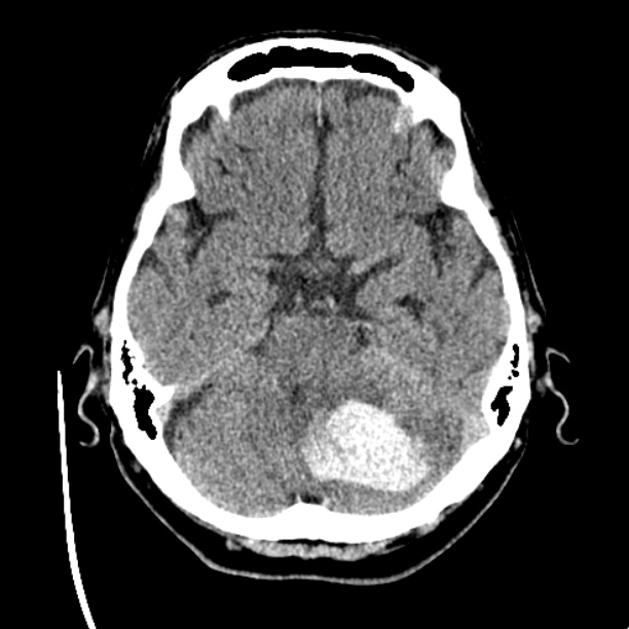
cerebellar haemorrhage usually presents with typical "posterior circulation symptoms" such as vertigo, ataxia, nausea and vomiting, and also headache 6
Pathology
Long-standing poorly-controlled hypertension leads to a variety of pathological changes in the vessels:
-
microaneurysms of perforating arteries (Charcot-Bouchard aneurysms)
small (0.3-0.9 mm) diameter
occur on small (0.1-0.3 mm) diameter arteries
-
distribution matches the incidence of hypertensive haemorrhages
80% lenticulostriate
10% pons
10% cerebellum
found in patients with hypertension
may thrombose, leak (see cerebral microhaemorrhages) or rupture 2
accelerated atherosclerosis: affects larger vessels
hyaline arteriosclerosis
hyperplastic arteriosclerosis: seen in very elevated and protracted cases
Radiographic features
Imaging findings will depend on the location and time since bleeding, which are covered in the intracerebral haemorrhage article.
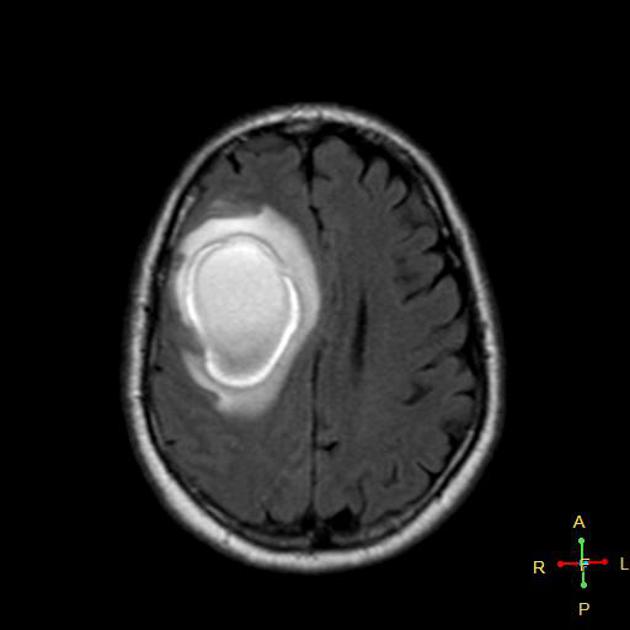
MRI
When hypertensive microangiopathy is present, multiple small areas of blooming artifact representing cerebral microhaemorrhages may be evident on GRE or SWI sequences in addition to the ICH.
Treatment and prognosis
Haemorrhage causes displacement of brain tissue, but once resorbed, the patient recovers with fewer deficits compared to similar-sized infarcts. Treatment of uncontrolled hypertension is very important to prevent recurrent ICH 7.
Characteristics of hypertensive haemorrhages that lead to poorer prognosis include 3:
bleed in the posterior fossa
large amount of mass effect
extension into the ventricular system







 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}